



- Download PDF
- |
- Download Citation
- |
- Email a Colleague
- |
- Share:
-
- Tweet
-
Journal of Vaccines & Immunization
Volume 3, Issue 4, October 2015, Pages 19–24
Short reportOpen Access
From package to protection: how do we close global coverage gaps to optimize the impact of vaccination?
-
Thomson A1,
Watson M1,
Picot V2,
Louis J2 and
Saadatian-Elahi M3,*

*Corresponding author: Dr. Mitra Saadatian-Elahi, Groupement Hospitalier Edouard Herriot, Service d’Hygiène, Epidémiologie et Prévention, Bâtiment 1, 5, place d'Arsonval; 69437 Lyon cedex 03, France. Tel.: +33 (0) 629364925; Fax: +33 (0) 472110726; E-mail: mitra.elahi@chu-lyon.fr
Received 10 June 2015 Revised 15 August 2015 Accepted 21 August 2015 Published 28 August 2015
DOI: http://dx.doi.org/10.14312/2053-1273.2015-4
Copyright: © 2015 Thomson A, et al. Published by NobleResearch Publishers. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
AbstractTop
The success of every vaccination program is dependent upon reaching and sustaining the target coverage rates. Vaccination programs are currently facing coverage gaps where target coverages are never reached and may also see erosion of coverage owing to, for example, loss of public confidence in vaccinations. The conference “From package to protection: how do we close global coverage gaps to optimize the impact of vaccination” gathered a multidisciplinary group of experts to explore the best options to address these gaps by challenging assumptions with evidence and focusing on impact. Within the broad challenge of increasing vaccine acceptance, there are many different circumstances depending on the disease, population demographics, culture and differences in health care systems. A basic requirement for addressing the coverage gap is to determine the relative contribution of each factor and to understand the underlying psychology of decision-making. Studies that aim at identifying and measuring drivers and barriers of vaccination, approaches to better understand the relative contribution of all possible determinants of vaccination uptake and evidence-based approaches to effective communication on vaccine risk and benefits were reviewed and discussed. The panel concluded that vaccination behaviour is a continuum phenomenon ranging from active demand to complete refusal of all vaccines and can vary through time, place and vaccine. Communication and interventional strategies should therefore be tailored by vaccine and population. Standardized and validated tools to measure the barriers and drivers of vaccine acceptance should be developed/tested and put together in a repository or "Matrix" of interventions to investigate the impact of intervention.
Keywords: Vaccine uptake; Immunization; vaccine coverage; barriers of vaccination; global coverage gaps; conference report
IntroductionTop
Despite the rapid progress in the provision of routine immunization that came after the introduction of the Expanded Program on Immunization (EPI), vaccine coverage in both the developed and developing world is still far from the expected/recommended rates. One in every 5 children born today never receives routine vaccine and an estimated 1.5 million children still die of vaccine-preventable diseases every year [1]. Poverty, ignorance and lack of access to health care facilities are among the obstacles for vaccination leading to suboptimal vaccine coverage. However, vaccination programs are also facing erosion of coverage owing to, for example, loss of public confidence in vaccination. The recent measles outbreaks in the UK are an example of a direct consequence of parental hesitation vis-à-vis the Measles-Mumps-Rubella (MMR) vaccination for their children due to concerns over the specific links with autism [2]. Coverage and erosion gaps exist in both low- and high-income countries and in child and adult vaccination programs.
There is widespread recognition of the urgent need to tackle these coverage gaps and erosion to enhance vaccination coverage rates. The conference "From package to protection – How do we close global coverage gaps to optimize the impact of vaccination?" held September 22-24, 2014 by the Foundation Mérieux (Annecy, France) aimed to explore how we can most effectively address these gaps by challenging assumptions with evidence and focusing on impact. A multidisciplinary group of international experts from academia, industry, international organizations, national authorities and public health institutes participated at the meeting to review and discuss various issues including: (i) The social and cognitive determinants of vaccination by examining studies that aim at identifying and measuring the drivers and barriers of vaccination, (ii) Approaches to better understand the relative contribution of all possible determinants of vaccination uptake in order to build practical intervention strategies that could influence vaccine coverage, (iii) Evidence-based approaches to effective communication on vaccine risk and benefits.
This report provides a summary of selected issues presented and discussed by the participants, the key findings and recommendations for future approaches to addressing this issue.
Social and cognitive determinants of vaccination
Individual attitude towards vaccination is a complex combination of several determinants such as beliefs, perceived severity of the disease, understanding of vaccine effectiveness, socioeconomic status, past experience, etc. which together converge to subjective judgement. The attitude of physicians with regard to vaccination and the role of the media could also influence individual attitudes. A better understanding of social and cognitive determinants of vaccination would make it possible to implement intervention strategies to optimize vaccine coverage.
The World Health Organization (WHO) Strategic Advisory Group of Experts (SAGE) developed a matrix based on three main groups of determinants of vaccine acceptance: contextual influence, individual and group influences and vaccination specific issues [3]. The matrix was used in a qualitative study among immunization managers in 13 WHO regions, mostly in low- and middle-income countries and provided evidence that vaccine hesitancy is an individual behaviour that results from many variables and factors such as religious beliefs, fear of adverse effects, geographic barriers, the influence of the media and the mode of vaccine delivery [4].
Another ongoing study is the VaxiTrends project, a collaborative and patient-centric project that aims to measure attitudes and perception towards vaccination, to understand the drivers and barriers of vaccination, to predict and impact vaccination uptake and to monitor through time and the population the impact of programs. The qualitative stage which involved three countries (France, USA and the UK), consisted in interviewing individuals about their experiences with flu and adult booster vaccination. The results showed that experience with each vaccine is highly individual and goes beyond socio-demographic factors. Non-vaccination was highly emotional (triggered by lack of perceived vulnerability and/or recommendation) while vaccination was more rational. The study identified many internal factors (socioeconomic status, health condition, personal experience, awareness and the perceived risk) and external factors (health-care provider recommendations, relatives, the media) that interact and influence an individual’s perception and acceptance of vaccination.
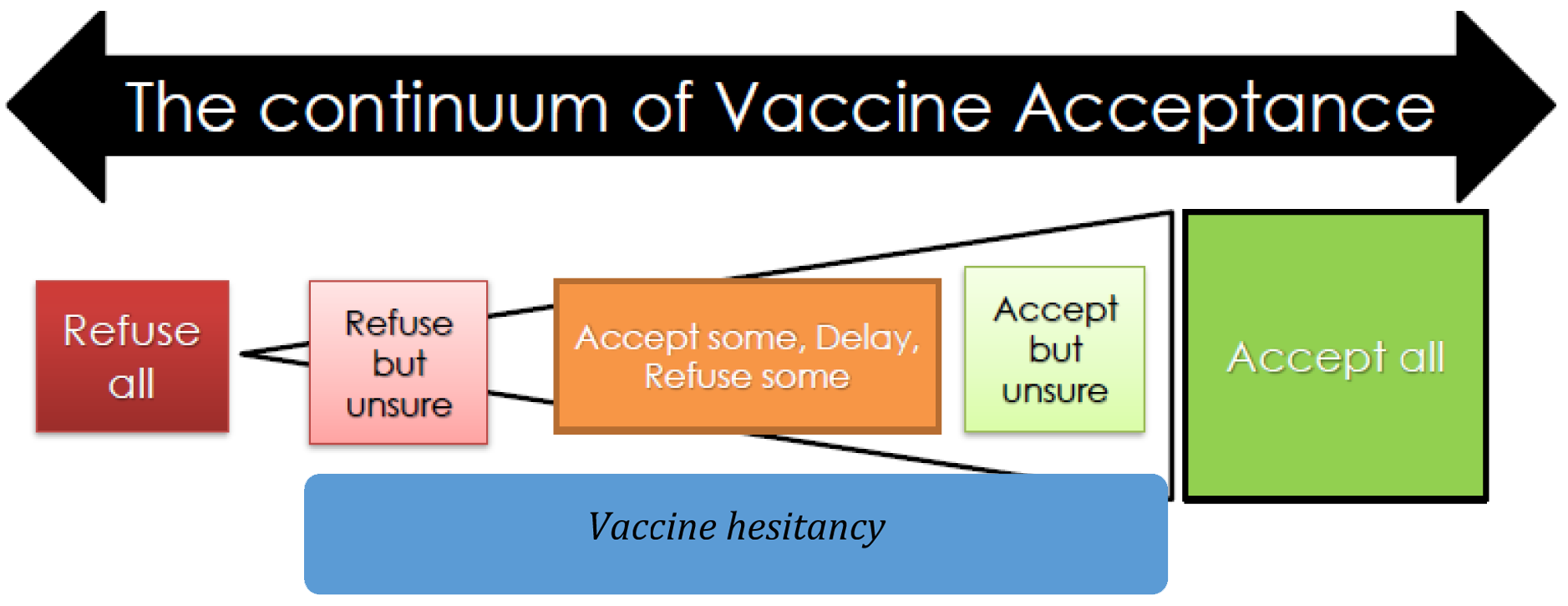
Beyond a rational "risk versus benefit" analysis, an individual's decisions about vaccination encompass different factors such as social norms, past experiences, emotions, values, conversations with friends and other day-to-day concerns about health and well-being. Decisions to use vaccination services are complex, multi-dimensional and can vary through time, place and vaccines. Attitudes to vaccination can therefore be considered as a continuum rather than a dichotomous (anti- versus pro-vaccine) belief. The continuum character of vaccine acceptance is now recognized by the introduction of the term "Vaccine hesitancy" that has recently been defined as "a delay in acceptance or refusal of vaccine despite availability and quality of vaccine services" (Figure 1). Vaccine hesitants are a heterogeneous group who may: (i) refuse all vaccines but are unsure; (ii) refuse some, delay and accept some; (iii) accept all but are unsure. Any effort to increase vaccine acceptance will therefore be more successful if it is founded on an understanding of underlying psychology of decision-making.
Measuring the drivers and barriers of vaccination
In many countries, there has been a shift in the traditional role of physicians as the principal deciders of patient care to shared decision-making between health-care providers (HCPs) and patients who want to be active partners in their health-related decisions. The attitudes of HCPs to vaccination and vaccine advocacy are therefore significant factors influencing the patient’s choice. The well-known low coverage rates of influenza vaccine among HCPs illustrate that this population can also be hesitant and consequently have negative impact on vaccine acceptance. Understanding the level of autonomous drivers and barriers in each group (patient and HCPs) is key to change vaccine behaviour. However, there is currently no validated tool for such purposes.
An alternative perspective consists in considering vaccination as a motivated decision. To further explore this possibility, the MoVac© and MoVAd© scales were developed with the aim to measure individual differences in dimensions related to intrinsic motivation to engage in a behaviour. A modified version of the MoVac© scale, adapted for influenza vaccination, was used in three hospitals in London to evaluate the motivation of HCPs to get vaccinated and to engage in vaccination advocacy and recommendation. Each scale had four components: (i) Is the vaccine effective? (ii) Is the vaccine meaningful? (iii) Do I have autonomy? and (iv) Am I competent? Overall, 1,670 subjects (70% female) answered the questionnaire. The highest vaccination uptake was reported among medical doctors, nurses and applied health professionals. Influenza vaccine effectiveness, meaningfulness and competence turned out to be the main drivers of motivation while autonomy showed the weakest association with the fact of being vaccinated. The study also investigated social and environmental influences on vaccination behaviour. HCPs were more likely to get vaccinated when they knew that their line manager was vaccinated.
Two ongoing studies that aimed at identifying and measuring the drivers and barriers of vaccination for parents were discussed during the conference. The Parent Attitudes about Childhood Vaccines (PACV) survey was developed to identify vaccine-hesitant parents and to investigate the effect of early effective communication strategy on their vaccine behaviour. The PACV scale included 15 items covering three domains related to behaviour, the safety and efficacy of vaccines and general attitudes. The scale ranged from zero to 100, the latter designating “very hesitant parents”. The PACV questionnaire was given to parents when their child was 2 months old and the immunization status of their children with regard to six vaccines was assessed 12 months later for those who completed the survey [5]. The results revealed the validity of the PACV score in predicting the parents who will have under-immunized children. Indeed, the parents who were identified as "hesitant" by the PACV score were more likely to have under-immunized children for 46.8% more days (95% CI, 40.3%-53.3%) than those who were identified as less hesitant [6]. The format in which providers initiated the vaccine discussion with parents was also shown to be a predictor of parental decision [6]. Indeed, a presumptive approach and provider pursuit of vaccine recommendation led to vaccine acceptance among 47% of initially resistant parents [6].
The Vaccine Attitudes Beliefs and Concerns (V-ABC) is a three-tiered measure designed to (i) conduct surveillance of population-level vaccine acceptance, (ii) identify key classes of attitudes, beliefs and concerns that affect vaccine acceptance and (iii) diagnose detailed influences in order to target, pre-test and evaluate public campaigns and other interventions. The proposed structure is to determine the Vaccine Acceptance Index (VAI) by using answers from a set of questions on vaccine safety, efficacy, cost, etc. The V-ABC framework is being tested among veterinary nurses in Australia to better understand their knowledge and attitudes towards Q-fever vaccination.
Approaches to better understand the determinants of vaccination uptake
As stated by the WHO, vaccine availability, physical access, social and community factors, parental and family factors, health worker factors and missed opportunities in health services are core problem areas that impact vaccination uptake (Figure 2). A better understanding of the relative contribution of each determinant is crucial for addressing coverage gaps. For this purpose, the WHO developed a diagnostic method (UnVacc) to analyse core problem areas preventing some children from being vaccinated. The UnVacc toolkit consists of a screening methodology to identify the broad core problem areas and strategies to address the problem.
In order to address the problems of vaccine availability, the WHO defined the Effective Vaccine Management strategy – a continuous quality improvement process including several components (stock management, maintenance, etc.) to be taken into consideration for the management of vaccine delivery.

As already mentioned, HCPs play an important role in vaccination uptake. It is therefore important to evaluate their ability to locate areas where educational efforts still need to be improved. For this purpose, the WHO developed the health worker Knowledge, Attitude and Practices (KAP) method which consists in observing vaccinator/care-giver interaction, interviews with vaccinators, supervisors, and care-givers and finally group discussion with care-givers who bring children in for vaccination. A literature review of the prevalence of missed opportunities in 0-to-18-year-old in developing countries showed that 40% of them could be addressed properly [7].
The community and society within which the unvaccinated children live could constitute another core problem area. For example, during the measles outbreak in Bulgaria, the highest incidence rates (579/10,000 population) were reported among the ethnic Roma minority [8]. To better understand and influence behaviour, the WHO developed the Targeting Immunization Programs (TIP) tool. The objective is to segment the population, refine problems, analyse behaviour, profile target groups and define targeted strategies and interventions.
The 5As Vaccination Coverage Root Cause Initiative is another methodology for evidence-based analysis of the coverage gap and the development of a strategic plan that targets the key determinants of poor uptake. This approach uses an alliterative taxonomy to facilitate a common understanding of the problem: access, affordability, awareness, acceptance and activation. A multi-sectorial working group makes a differential diagnosis of the ‘A’ that accounts for suboptimal coverage through an in-depth situation analysis drawing upon data from the national immunization program, vaccination impact, media and social analytics, behavioural studies, ongoing best practices, and the knowledge and insights of the working group members and other key stakeholders. The 5As analytical tool is composed of four phases: scope and working group engagement, analysis, strategy and action plan development and implementation. Currently, four pilots are underway in Romania (flu), Mexico (flu), Gabon (EPI), and Russia (primary series).
As mentioned earlier, vaccine acceptance relates to parental concerns about the real benefits and safety of vaccines. Well-organized dialogues between health providers and parents are therefore paramount. Several approaches have been investigated to address acceptance [9-11]. The vaccine acceptance spectrum includes five categories: ‘unquestioning acceptor’ (30–40%), the ‘cautious acceptor’ (25–35%); the ‘hesitant’ (20–30%); the ‘late or selective vaccinator’ (2–27%); and the ‘refuser’ of all vaccines (<2%) [10]. The Strategies And Resources for Assisting Hesitant parents with immunization (SARAH) is a framework to guide health professionals in communicating with each category of parents. The framework is based on several major points i.e. identify parental position, undertake a flexible approach and communication style and finally, tailor the right resources [12]. The quality of communication is also a critical factor. Poor communication can contribute to rejection of vaccinations or dissatisfaction with care. Barriers to effective communication could be systemic (i.e. insufficient, uncertain and changing information), related to the communicator (insufficient knowledge of what consumers know) or to the patient (lack of comprehension and use of information). The evidence-based strategies that lead to the best communication include (i) providing numbers, (ii) reducing consumer cognitive effort, (iii) providing effective cues especially when numeric information is unfamiliar, (iv) directing attention to the most important information and (v) setting-up appropriate systems to assist consumers [13-14].
To really understand and address the social and behavioural determinants of vaccine acceptance, the input of some very diverse disciplines (social sciences, cognitive psychology, communication sciences) is required, many of which are not currently collaborating. This has meant that the body of knowledge is scattered and therefore, many practices are not evidence-based. MotivGate [15] is a community of practice which aims to provide a place to share and generate evidence-based research and proven practical intervention. It is built collectively by community members who share knowledge and topics related to vaccination acceptance (papers, reports, interventions, etc.) via a dynamic document.
Social and behavioural change interventions
Decision-making on vaccination is driven by conscious, subconscious and unconscious beliefs that can be mechanical (i.e. culture-oriented), energetic, interpersonal, or transcendental. Thus, the success of vaccination requires (i) addressing people’s beliefs in daily routine practice to help them to make wise decisions, (ii) bringing together the child and family, the HCPs and the immunization systems, (iii) drawing messages that are effective in overcoming parental reluctance to vaccinate and (iv) disseminating these messages through the most trusted source of information.
People often have inaccurate factual beliefs – some are uninformed and some are misinformed. Misinformation about vaccine may contribute to hesitancy and under-vaccination. A good example is given by the MMR vaccine and its discredited link with autism that led to a decrease in vaccination coverage in several countries around the world. Using motivated reasoning, a nationally representative study in the USA investigated the effectiveness of messages to reduce MMR vaccine misperception. Four information approaches were tested: (i) correcting misinformation, (ii) presenting information on disease risk, (iii) using dramatic narratives, or (iv) presenting disease dangers through images [16]. None of the approaches increased intent to vaccinate with MMR. The authors concluded that pro-vaccine messages are an ineffective approach to countering misperceptions about vaccines and trying to scare parents can make the problem worse in some cases. These findings emphasize the importance of testing messages before their dissemination. Different sources of information may have different credibility and it is important to take into consideration the role of each source. Paediatricians have been reported as the most trusted source for vaccine safety information (76%) followed by other health care providers (26%) and government vaccine experts/officials (23%) [17].
Vaccine exemption policies may also influence vaccine coverage rate. Ease of obtaining vaccine exemption (incidence rate ratio = 1.53; 95% confidence interval, 1.10-2.14) and availability of personal belief exemptions (incidence rate ratio = 1.48; 95% confidence interval, 1.03-2.13) were significantly associated with a higher incidence of pertussis in the United States [18]. Mandatory vaccinations to enter school together with a rational administrative requirement to grant exemptions and informed dissent could be an intervention strategy to increase vaccination coverage.
Following the H1N1 epidemic in 2009, several publications provided arguments that pregnant women should no longer be systematically excluded from at least some vaccination programs. In an effort to promote the immunization of pregnant women, a randomised evaluation of a comprehensive intervention, the “P3” package (Practice, Provider and Patient-based) is ongoing in Georgia. The objective is to evaluate the effectiveness of this intervention package on increasing influenza and Tdap vaccine acceptance among pregnant women. Package intervention could also be beneficial for developing countries. An intervention package is ongoing in Pakistan to improve vaccine coverage for pneumococcal vaccine in children.
Another potential intervention strategy is an effective provider-parent communication tool. The Motivational Interviewing approach is a person-centred, collaborative and evocative particular sort of conversation between HCPs and their patients. The central concept of such an approach is the identification, examination and resolution of ambivalence about changing behaviour. It is designed to strengthen an individual’s motivation for and movement toward a specific goal by eliciting and exploring the person’s own arguments for change.
There is need to build a relationship of trust and transparency and give science a face and a personality. This has been shown in Belgium where a new guideline on whooping cough vaccination came out following the intervention of parents who lost a child owing to this vaccine-preventable disease, emphasizing the fact that the most impactful talks could be the least factual. Similarly, in Australia in 2011, an Immunization Alliance supported by parents carried out a campaign on immunization [19]. A survey conducted by the Alliance found that the campaign prompted approximately one-third of the parents who had doubted, had safety concerns or even refused vaccines to think and feel more positively about them. The next step of this survey is to conceptualize hesitant communities and to investigate how hesitancy is formed, sustained and resisted within communities.
After reviewing the current situation, the expert panel identified the following lessons learnt and the main challenges to be addressed with high priority:
Lessons learnt: Drivers and barriers are vaccine-dependant and should therefore be addressed by vaccine and population to tailor responses. Communication between HCPs and public is crucial, (i) HCPs are still key to decision-making. We must insure that they have the appropriate and essential skill set to communicate with the public by providing adequate and straightforward information that will help them to decide for themselves, (ii) The public increasingly asks to be active partners in their decisions to be vaccinated and/or to vaccinate their children. To ensure actions that guarantee better vaccination acceptance, dialogue needs to be tailored according to the public’s needs and expectations, (iii) Public health needs effective health promotion, not just communication of facts. The public is relatively unmoved by data. Thus, effective and evidence-based behaviour to change communications is required to improve vaccine acceptance.
Challenges: (i) Foster a dynamic, multidisciplinary and better connected community of practice, (ii) Establish vaccination acceptance as a legitimate discipline for theoretical and applied research, (iii) Ensure adoption of standardised and validated tools to measure barriers and drivers of vaccine acceptance and the impact of intervention, (iv) Bring all tools and manuals together into a repository or "Matrix" of interventions, (v) Produce rigorous qualitative, quantitative, culturally and geographically balanced evidence-based data on drivers and barriers to coverage and acceptance; intervention options; and measuring impact of interventions, (vi) Develop better behaviour to change communication strategies.
ConclusionTop
Vaccination acceptance is mediated by a complex mix of socio-demographic and socio-psychological factors. There is a need for robust and collaborative research across a number of disciplines to develop the tools that can allow us to better understand and measure these determinants in different contexts, and to design and test interventions that could increase confidence in vaccination.
Acknowledgments
The authors express their gratitude to all of the speakers who shared their findings (Annex 1, list of speakers and participants). Thanks are also due to Sanofi Pasteur for sponsoring the meeting, to the Mérieux Foundation Conference Centre for outstanding local organization and to Ms. Cindy Grasso for the logistical aspects.
Financial disclosure
Authors have no financial relationship relevant to this article to disclose.
Abbreviations
EPI: Expanded Program on Immunization; DTP3: Diphtheria-tetanus-pertussis; MMR: Measles-Mumps-Rubella; HCPs: Health Care Providers; WHO: World Health Organization; SAGE: Strategic Advisory Group of Experts; PACV: Parent Attitudes about Childhood Vaccines; V-ABC: Vaccine Attitudes Beliefs and Concerns; VAI: Vaccine Acceptance Index; RED: Reaching Every District; KAP: Knowledge, Attitude and Practices; TIP: Targeting Immunization Programs; SARAH: Strategies And Resources for Assisting Hesitant parents with immunization.
Supplementary data
Annex 1
ReferencesTop
[1]WHO, UNISEF, World Bank. States of the world’s vaccines and immunization, 3rd edition. Geneva. World Health Organization. 2009.Article
[2]McHale P, Keenan A, Ghebrehewet S. Reasons for measles cases not being vaccinated with MMR: investigation into parents and carers views following a large measles outbreak. Epidemiol Infect. 2015; 12:1-6.Article Pubmed
[3]The SAGE Vaccine Hesitancy Working Group. What influences vaccine accep-tance: A model of determinants of vaccine hesitancy. 2013[cited November 6th, 2013].Article
[4]Dubé E, Gagnon D, Nickels E, Jeram S, Schuster M. Mapping vaccine hesitancy-country-specific characteristics of a global phenomenon. Vaccine. 2014; 32(49):6649-6654.Article Pubmed
[5]Opel DJ, Heritage J, Taylor JA, Mangione-Smith R, Salas HS, et al. The architecture of provider-parent vaccine discussions at health supervision visits. Pediatrics. 2013; 132(6):1037-1046.Article Pubmed
[6]Opel DJ, Taylor JA, Zhou C, Catz S, Myaing M, et al. The relationship between parent attitudes about childhood vaccines survey scores and future child immunization status: a validation study. JAMA Pediatr. 2013; 167(11):1065-1071.Article Pubmed
[7]Sridhar S, Maleq N, Guillerment E, Colombini A, Gessner BD. A systematic literature review of missed opportunities for immunization in low- and middle-income countries. Vaccine. 2014; 32(51):6870-6879.Article Pubmed
[8]Kojouharova M. Measles outbreak in Bulgaria, 2009-2010. National center of infectious and parasitic diseases, Bulgaria (Accessed on 3 January 2015) .Article
[9]Williams SE. What are the factors that contribute to parental vaccine-hesitancy and what can we do about it. Hum Vaccin Immunother. 2014; 10(9):2584-2596.Article Pubmed
[10]Kaufman J, Synnot A, Ryan R, Hill S, Horey D, et al. Face to face interventions for informing or educating parents about early childhood vaccination. Cochrane Database Syst Rev. 2013; 5:CD010038.Article Pubmed
[11]Sadaf A, Richards JL, Glanz J, Salmon DA, Omer SB. A systematic review of interventions for reducing parental vaccine refusal and vaccine hesitancy. Vaccine. 2013; 31(40):4293-4304.Article Pubmed
[12]Leask J, Kinnersley P, Jackson C, Cheater F, Bedford H, et al. Communicating with parents about vaccination: a framework for health professionals. BMC Pediatr. 2012; 12:154.Article Pubmed
[13]Peters E, Hart PS, Tusler M, Fraenkel L. Numbers matter to informed patient choices: a randomized design across age and numeracy levels. Med Decis Making. 2014; 34(4):430-442.Article Pubmed
[14]Peters E, Hart PS, Fraenkel L. Informing patients: the influence of numeracy, framing, and format of side effect information on risk perceptions. Med Decis Making. 2011; 31(3):432-436.Article Pubmed
[16]Nyhan B, Reifler J, Richey S, Freed GL. Effective messages in vaccine promotion: a randomized trial. Pediatrics. 2014; 133(4):e835-842.Article Pubmed
[17]Freed GL, Clark SJ, Butchart AT, Singer DC, Davis MM. Sources and perceived credibility of vaccine-safety information for parents. Pediatrics. 2011; 127 Suppl 1:S107-112.Article Pubmed
[18]Omer SB, Pan WK, Halsey NA, Stokley S, Moulton LH, et al. Nonmedical exemptions to school immunization requirements: secular trends and association of state policies with pertussis incidence. JAMA. 2006; 296(14):1757-1763.Article Pubmed
[19]Immunization alliance in Western Australia. (Accessed on 3 January 2015).Article
 Copyright
© 2012-2019 NobleResearch Group. All Rights Reserved
Copyright
© 2012-2019 NobleResearch Group. All Rights Reserved