



- Download PDF
- |
- Download Citation
- |
- Email a Colleague
- |
- Share:
-
- Tweet
-
Journal of Radiology and Imaging
Volume 1, Issue 6, December 2016, Pages 39–43
Original researchOpen Access
A representative study of pediatric panoramic and cephalometric radiation exposure to organs of the head and neck
-
Evanthia Peikidis1,
Arthur D. Goren2,3,*
 ,
Richard D. Faber1,
Iryna Branets1,
Lawrence T. Dauer4,5,
Brian Quinn5 and
Dan Colosi2
,
Richard D. Faber1,
Iryna Branets1,
Lawrence T. Dauer4,5,
Brian Quinn5 and
Dan Colosi2
*Corresponding author: Arthur D. Goren, Department of Cariology and Comprehensive Care, College of Dentistry, New York University, New York, USA; E-mail: ag153@nyu.edu
Received 30 August 2016 Revised 25 October 2016 Accepted 10 November 2016 Published 25 November 2016
DOI: http://dx.doi.org/10.14312/2399-8172.2016-9
Copyright: © 2016 Peikidis E, et al. Published by NobleResearch Publishers. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
AbstractTop
The purpose of this study was to measure juvenile patient radiation dose to organs of the head and neck during digital panoramic and cephalometric radiography using anthropomorphic CIRS phantoms at 5 and 10-years-old with nanoDot optically stimulated luminescent dosimeters (OSLDs). OSLDs were placed at 21 head and neck organ sites of the phantom heads. Phantom heads were subjected to panoramic and cephalometric imaging protocols using manufacturers’ predefined exposure settings. Radiation dose fractions to various organ sites were determined using reference values from the ICRP-89 document. Organ equivalent doses and overall effective doses were based on ICRP-103 tissue weighting factors. Overall measured organ doses were higher for the 5-year-old than for the 10-year-old for both the panoramic and the cephalometric imaging protocols. The highest doses seen were in the salivary glands, extrathoracic airway, and the oral mucosa. The organ equivalent dose in microsieverts (µSv) also yielded similar results. The effective dose for the 5-year-old was 27.8 µSv for the panoramic and 6.5 µSv for the cephalometric, while the 10-year-old results were 26.3 µSv for the panoramic and 3.8 µSv for the cephalometric. The effective doses estimated for this study for the 5-year-old and 10-year-old during cephalometric procedures are lower than the US natural background reading of 8.5 µSv per day and lower than the US average exposure per day of 17 µSv. The effective doses estimated in this study for the panoramic procedure for both phantoms were above the natural background and above the national average per day. These data support the notion that child-appropriate technique factors and geometry factors should be used for panoramic and cephalometric imaging protocols.
Keywords: juvenile patient radiation; effective dose; panoramic radiation; cephalometric radiation; equivalent dose
Background informationTop
Panoramic and cephalometric radiography are used in orthodontics for the diagnosis, treatment planning, and re-evaluation of patients. These radiographs may be taken at the initial visit, during treatment to evaluate progress, and at the conclusion to evaluate success of reaching treatment goals. There is a distinct paucity of radiation dosimetry data on juveniles. Digital panoramic and cephalometric exposure to various organ sites has previously been measured with adult Rando phantom heads using thermo-luminescent dosimeters (TLDs). However, to our knowledge, no other investigators have used juvenile CIRS phantoms either with optically stimulated luminescent dosimeters (OSLDs) or TLDs to measure radiation exposure. CIRS phantoms are anthropomorphic, cross-sectional phantoms designed specifically to investigate organ radiation doses [1]. OSLDs have improved measurement sensitivity at low radiation doses [2].
Since 1928, the International Commission on Radiological Protection (ICRP) has developed radiological protection standards, guidelines, and practices to follow in order to minimize the risk of cancer and genetic diseases, and to decrease the harmful effects of ionizing radiation [3]. The ICRP uses the equivalent and effective dose (measured in microsieverts) to determine the stochastic risks from radiation exposure, which is the probability of cancer induction and genetic damage [4, 5]. The equivalent dose takes into account the type of ionizing radiation producing the dose, while the effective dose is the tissue-weighted sum of the equivalent doses in all specified tissues and organs of the body [5-7].
Although the amount of radiation per digital panoramic and cephalometric radiograph is relatively small, radiation doses from imaging procedures performed throughout treatment are cumulative. Current imaging guidelines recommend that clinicians develop adequate justification prior to exposing a patient to radiation [8, 9]. This is based on the specific objectives of the exposure in relation to the history and clinical examination of the patient, as well as the findings on previous radiographs. The benefits of obtaining diagnostic information should outweigh the negative effects from the exposure. Justification is especially important in children. Children are more sensitive to this radiation compared to adults, because of their smaller size and ongoing development of their cells, tissues, and organs [10].
Previous studies measuring digital panoramic and cephalometric radiation doses to phantom heads have used TLDs on adult phantom heads, a majority being Rando phantoms. In this study, we used OSLDs on juvenile CIRS phantoms to measure radiation exposure. OSLDs are a more advanced type of dosimeter (Figure 1). OSL dosimeters when analyzed use only a fraction of the stored charge so that re-analysis is possible, instead of heat, light is used and is easier to control and the material used for dosimetry is sapphire which is very rugged with little to no post irradiation fading [11-13].
Anthropomorphic phantoms are available in sizes and conformations that range from newborn to adult. They differ from other reference phantoms in that the sectional surfaces are extremely flat and smooth due to epoxy base materials and do not require any special coating or treatment [1]. This results in increased accuracy due to minimal air interfaces between the sections. They also differ from other phantoms by providing optimized OSLD locations specific to 22 radiosensitive inner organs for precise calculations using the minimum number of detectors necessary [1]. CIRS tissue-equivalent epoxy resins and bone formulations offer superior tissue simulation and lifelike imaging properties compared to other phantoms used in other studies [1].
Little absorbed dose data obtained with juvenile CIRS anthropomorphic phantoms and nanoDot OSLDs are available for digital panoramic and cephalometric radiographic examinations. The objective of this study was to characterize juvenile patient radiation dose to organs of the head and neck during digital panoramic and cephalometric radiography using nanoDot OSLDs and juvenile CIRS phantoms that model the radiation absorption characteristics of a 5-year-old and a 10-year-old male child. The data were obtained using a commercially available panoramic-cephalometric unit and the manufacturer’s exposure settings.
Materials and methodsTop
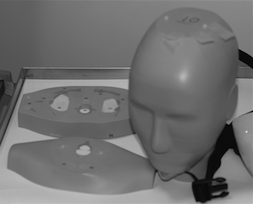
Two phantom heads were used: a child male anthropomorphic phantom (model 705; Computerized Imaging Reference System, Norfolk, Va) corresponding to an average 5-year-old boy who is 110cm in height and 19 kg in weight and a child male anthropomorphic phantom (model 706; Computerized Imaging Reference System) corresponding to an average 10-year-old boy who is 140 cm in height and 32 kg in weight (Figure 2, Anthropomorphic phantom head). OSL dosimeters were placed at the location of 21 key head and neck organs in the two phantom heads to assess the radiation doses (Figure 3, Optically stimulated luminescent dosimeter slots in the phantom head). An Instrumentarium OP100D Orthopantomograph and cephalometric unit (Instrumentarium Imaging, Tuusula, Finland) was used in this study to expose the phantoms. Preset pediatric settings were used with the child phantom heads. The parameters used were 73 kVp, 6.4 mA, and 16.8 s for the panoramic and 85 kVp, 12 mA, and 17.6 s for the cephalometric protocol. Table 1 shows the parameters used. Experimental methods were as described by Najjar et al., [14]. Each phantom was exposed three times for each protocol, and radiation exposure values to the OSLDs were read. The dosimeters were pre-read before the experiment using a MicroStar Reader (Landauer, Glenwood, Ill.) to determine the baseline recorded exposure. Following each imaging protocol, dosimeters were read three times, and the baseline recorded exposure was subtracted from the averaged readings. All dosimeters were calibrated for the study. Data analysis was performed using Microsoft Excel (Microsoft, Redmond, Wash). Equivalent doses were calculated using the tissue weighting factors of the 2007 ICRP’s recommendations [6]. Organ fractions, and organ equivalent doses and overall effective doses, were calculated using values from ICRP-89 and ICRP-103, respectively [15, 16].

| Image type | Paranomic | Lateral cephalometric |
| Voltage (kVp) | 73 | 85 |
| Current (mA) | 6.4 | 12 |
| Time (s) | 16.8 | 17.6 |
ResultsTop
Overall measured organ doses were higher for the 5-year-old than for the 10-year-old for both the panoramic and the cephalometric imaging (Table 2 and 3). The highest doses were measured in the salivary glands, extrathoracic airway, and the oral mucosa. The organ equivalent dose in micro Sieverts also yielded similar results (Tables 4 and 5). The effective dose in micro Sieverts for the 5-year-old was 27.8 for the panoramic and 6.5 for the cephalometric, while the 10-year-old results were 26.3 for the panoramic and 3.8 for the cephalometric (Tables 6 and 7).
| Average organ dose* panorex | Organ dose (µGy) 5-year-old | Organ dose (µGy) 10-year-old |
| Bone marrow | 4.3E + 00 | 4.5E + 00 |
| Bone surface | 1.8E + 01 | 8.9E + 00 |
| Brain | 1.3E + 0.1 | 9.1E + 00 |
| Calvarium | 3.2E + 00 | 2.6E + 00 |
| Cervical spine | 1.1E + 00 | 1.0E + 00 |
| Esophagus | 4.0E + 00 | 7.8E + 00 |
| Extratoracic airway** | 6.3E + 0.1 | 1.2E + 01 |
| Lens | 1.9E + 01 | 1.1E + 01 |
| Lymphatic nodes | 4.6E + 00 | 4.4E + 00 |
| Mandible | 9.9E + 00 | 4.4E + 00 |
| Muscle | 4.6E + 00 | 5.0E + 02 |
| Oral mucosa** | 1.5E + 02 | 1.4E + 02 |
| Parotid | 1.5E + 02 | 1.9E + 02 |
| Salivary glands** | 4.4E + 02 | 3.5E + 02 |
| Skin | 2.6E + 01 | 1.2E + 01 |
| Sublingual | 1.5E + 02 | 7.8E + 01 |
| Submandibular | 1.5E + 02 | 7.8E + 02 |
| Thyroid | 2.0E + 01 | 3.9E + 01 |
| Average organ dose* Rt Lat Ceph | Organ dose (µGy) 5-year-oldd | Organ dose (µGy) 10-year-old |
| Bone marrow | 3.8E + 00 | 2.9E + 00 |
| Bone surface | 8.9E + 00 | 1.2E + 00 |
| Brain | 9.1E + 00 | 2.8E + 01 |
| Calvarium | 2.6E + 00 | 2.3E + 00 |
| Cervical spine | 1.0E + 00 | 4.0E - 01 |
| Esophagus | 7.8E + 00 | 1.2E + 00 |
| Extratoracic airway** | 6.3E + 01 | 1.3E + 01 |
| Lens | 1.9E + 01 | 1.4E + 01 |
| Lymphatic nodes | 1.1E + 00 | 6.0E - 01 |
| Mandible | 3.0E - 01 | 1.0E - 01 |
| Muscle | 1.0E - 01 | 1.0E - 01 |
| Oral mucosa** | 2.8E + 01 | 1.3E + 01 |
| Parotid | 3.8E + 01 | 1.7E + 01 |
| Salivary glands** | 7.2E + 01 | 3.3E + 01 |
| Skin | 1.0E + 00 | 9.0E - 01 |
| Sublingual | 1.7E + 00 | 8.1E + 00 |
| Submandibular | 1.7E + 01 | 8.1E + 00 |
| Thyroid | 6.6E + 00 | 6.1E + 00 |
| Equivalent dose* panorex | Organ equivalent dose (µSv) 5-year-old | Organ equivalent dose (µSv) 10-year-old |
| Bone marrow | 5.2E - 01 | 5.2E - 01 |
| Bone surface | 1.8E - 01 | 8.9E - 02 |
| Brain | 1.3E - 01 | 9.3E - 02 |
| Esophagus | 1.6E - 01 | 3.1E - 01 |
| Lens | 1.9E + 01 | 1.0E + 01 |
| Salivary glands | 4.4E + 00 | 3.5E + 00 |
| Skin | 2.6E - 01 | 1.1E - 01 |
| Thyroid | 7.8E - 01 | 1.6E + 00 |
| Remainder | 2.1E + 01 | 2.1E + 01 |
| Equivalent dose* Rt Lat Ceph | Organ equivalent dose (µSv) 5-year-old | Organ equivalent dose (µSv) 10-year-old |
| Bone marrow | 4.5E - 01 | 3.4E - 01 |
| Bone surface | 1.6E - 02 | 1.2E - 02 |
| Brain | 2.8E - 01 | 2.8E - 01 |
| Esophagus | 5.3E - 02 | 4.8E - 02 |
| Lens | 1.9E + 01 | 1.4E + 01 |
| Salivary glands | 7.2E - 01 | 3.3E - 01 |
| Skin | 1.0E - 02 | 9.3E - 03 |
| Thyroid | 2.6E - 01 | 2.4E - 01 |
| Remainder | 4.8E + 00 | 2.5E + 00 |
| Effective dose (µSv) panorex 5-year-old | Effective dose (µSv) panorex 10-year-old |
| 27.8 µSv | 26.3 µSv |
| Effective dose (µSv) Lat Ceph 5-year-old | Effective dose (µSv) Lat Ceph 10-year-old |
| 6.5 µSv | 3.8 µSv |
DiscussionTop
To our knowledge, there are no published data from OSLD radiation dose measurements on CIRS juvenile anthropomorphic phantoms during digital panoramic and cephalometric imaging. CIRS phantoms are fabricated using materials that are superior in their imaging properties, and may more accurately simulate the radiation absorption characteristics of actual organs and tissues compared to the Rando phantom heads [1]. OSLDs are based on a more recent technology for measuring absorbed radiation, and recent studies appear to indicate that they have a higher sensitivity in the low radiation dose range [2, 13]. The aim of our study was to measure radiation exposure to different organs of the head and neck in juvenile phantoms using these recent technologies in combination. The data were obtained from a panoramic and cephalometric unit using the settings recommended by the manufacturer.
In our study, during the panoramic image, the effective dose in microsieverts was 27.8 for the 5-year-old and 26.3 for the 10-year-old. These values are slightly higher than measurements found in other studies using the Rando adult phantoms and TLDs [6, 17-21]. In a study by Davis et al., [22] the effective dose measured using a short collimator was 7.7 microsieverts. In general the higher values found in the 5-year-old phantom compared to the 10-year-old phantom in our study, and the adult phantoms in other studies, can be explained by the smaller organ size and by the increased sensitivity of a child’s developing organs and tissues to ionizing radiation. In children, their smaller cross-sectional area, the increased sensitivity of their tissues and organs to radiation, and their longer life expectancy, increases their cancer risk compared with adults [23]. A study by Ludlow et al., found that children are 2-5 times more sensitive to radiation carcinogenesis than adults [24]. The study also found that on average, the effective doses were 36% greater in child phantoms than adult phantoms [24].
In our study, during the cephalometric image, the effective dose in microsieverts was 6.5 for the 5-year-old and 3.8 for the 10-year-old. These values are in the range of values found in other studies using Rando phantoms and TLDs [6, 18, 19].
Different phantoms and dosimeter types used across studies may contribute to the differences in the obtained data. In a study by Gijbels et al., there was a wide range of patient radiation doses found for different panoramic units [25].
Different settings greatly impact the amount of radiation delivered when using panoramic systems on children. A study done by Davis et al., found that a short collimator should be used, and settings should produce a reduced exposure time and allow for reduction of tube current. Protocol selection should also provide flexibility for focal trough size, shape, and position to match the smaller head size [22]. A study done by Hayakawa et al., found that when lower kVp or mA settings were used for the Orthophos P10 and the PM 2002 CC panoramic units, absorbed doses were effectively reduced for all combinations of machines, programs, and detectors [9]. It can be concluded that panoramic systems, when used for children, should have settings specifically designed for imaging small heads.
The organs that received the highest radiation dose were the oral mucosa, extrathoracic airway, and the salivary glands. Studies done by Lecomber et al., and Gijbels et al., found that salivary glands received the most radiation during a dosimetry study of digital panoramic imaging [25, 26]. In another study by Visser et al., the highest absorbed doses were recorded at the parotid glands [27].
The organ of particular interest in radiation exposure in children is the thyroid gland. In 2003, the National Council on Radiation Protection and Measurement (NCRP) stated that the thyroid gland, especially in children, is among the most sensitive organs to radiation-induced tumors [28]. They recommended that thyroid shielding shall be provided for children, and should be provided for adults, when it will not interfere with the examination. This is important because more neck structure is exposed, and the thyroid is positioned higher in the neck in children than adults [29]. Future studies based on our paper can evaluate the effect of thyroid shielding on radiation doses to the thyroid during panoramic and cephalometric imaging.
The effective doses estimated for this study, 3.8 µSv for the 10-year-old and 6.5 µSv for the 5-year-old, during cephalometric procedures, are lower than the average natural background reading in the United States of 8.5 µSv per day and lower than the United States average exposure per day of 17 µSv [5]. The effective doses estimated in this study for the panoramic procedure was 27.8 µSv for the 5-year-old and 26.3 µSv for the 10-year-old.
Future studies that may add to these data include studying various exposure settings to determine if both organ equivalent and effective dose results can be reduced while maintaining the image quality needed for diagnostic evaluation. This will allow clinicians to follow the recommended “As Low as Reasonably Achievable” (ALARA) principles when using digital panoramic and cephalometric radiography. Evaluating the effects of body mass index, ethnicity, and sex on the effective doses can also add important information to this subject.
This was the first study to evaluate radiation exposure to juvenile CIRS anthropomorphic phantoms using nanoDot OSLDs in conjunction with digital panoramic and cephalometric imaging to provide organ equivalent doses and overall effective doses for 5-year-old and 10-year-old based on the latest ICRP-103 tissue weighting factors. An objective of an active dental quality assurance program is to insure that doses are kept ALARA while maintaining the necessary diagnostic information.
ConclusionTop
Child-appropriate technique factors (i.e. a reduction in exposure time) and geometry factors should be employed for appropriately justified procedures. In this study, the use of the CIRS phantoms in combination with the OSLDs resulted in estimates that were in the range of previous studies. In all cases, the organs that received the highest radiation dose were the oral mucosa, extrathoracic airway, and the salivary glands.
Conflicts of interest
The authors declare no conflicts of interest.
ReferencesTop
[1]CIRS Tissue Simulation & Phantom Technology. ATOM Dosimetry Phantoms Models 701-706. Norfolk, Virginia. 2013; 1–15.
[2]Branets I, Colosi DC, Branets L, Quinn B, Dauer LT, et al. Optically stimulated luminescence and thermoluminescence dosimetry: An overall perspective. Research. 2014; 1:720.Article
[3]Committee on the Biological Effects of Ionizing Radiations. Board of radiation effects, research division on earth and life studies, National Research Council of the National Academies. Health effects of exposure to low levels of ionizing radiation: BEIR V. National Academy of Sciences, Washington DC: National Academies Press. 1990.
[4]1990 recommendations of the International Commission on Radiological Protection. Ann ICRP. 1991; 21:1–201.Article Pubmed
[5]Pharoah M, White SC. Oral Radiology: Principle and Interpretation. 6th edition. St Louis, Mo.: Mosby. 2009.
[6]Ludlow JB, Davies-Ludlow LE, White SC. Patient risk related to common dental radiographic examinations: The impact of 2007 International Commission on Radiological Protection recommendations regarding dose calculations. J Am Dent Assoc. 2008; 139(9):1237–1243.Article Pubmed
[7]Brenner DJ. Effective dose: A flawed concept that could and should be replaced. Br J Radiol. 2008; 81(967):521–523.Article Pubmed
[8]The Royal College of Radiologists, Society and College of Radiographers, Institute of Physics and Engineering in Medicine. A guide to understanding the Implications of the ionizing radiation (medical exposure) regulations in radiotherapy. London: The Royal College of Radiologists. 2008.Article
[9]Hayakawa Y, Kobayashi N, Kuroyanagi K, Nishizawa K. Paediatric absorbed doses from rotational panoramic radiograph. Dentomaxillofac Radiol. 2001; 30(5):285–292.Article Pubmed
[10]Committee to Assess Health Risks from Exposure to Low Levels of Ionizing Radiation; Board of Radiation Effects, Research Division on Earth and Life Studies, National Research Council of the National Academies. Health risks from exposure to low levels of ionizing radiation: BEIR VII, Phase 2. National Academy of Sciences. Washington DC: National Academies Press. 2006.Article
[11]Lian OB. Luminescence dating: optically stimulated luminescence. Encyclopedia of quaternary science. University of London, UK: Royal Holloway. 2007; 1491–505.
[12]Zacharias N, Stuhec M, Knezevic Z, Fountoukidis E. Michael CT, Bassiakos Y. Low dose environmental dosimetry using thermo- and optically stimulated luminescence. Nucl Instrum Methods Phys Res A. 2007; 580:698–701.Article
[13]Dunn L, Lye J, Kenny J, Lehmann J, Williams I, Kron T. Commissioning of optically stimulated luminescence dosimeters for use in radiotherapy. Radiat Meas. 2013; 51-52:31–39.Article
[14]Najjar A, Colosi D, Dauer LT, Prins R, Patchell G, et al. Comparison of adult and child radiation equivalent doses from two dental cone-beam computed tomography units. Am J Orthod Dentofacial Orthop. 2013; 143(6):784–792.Article Pubmed
[15]Basic anatomical and physiological data for use in radiological protection reference value. ICRP Publication 89. Ann ICRP. 2002; 32 (3-4):5–265.Article Pubmed
[16]The 2007 Recommendations of the International Commission on Radiological Protection. ICRP publication 103. Ann ICRP. 2007; 37(2-4):1–322.Article
[17]Ludlow JB, Davies-Ludlow LE, Brooks SL. Dosimetry of two extraoral direct digital imaging devices: NewTom cone beam CT and Orthophos Plus DS panoramic unit. Dentomaxillofac Radiol. 2003; 32(4):229–234.Article Pubmed
[18]Ngan DC, Kharbanda OP, Geenty JP, Darendeliler MA. Comparison of radiation levels from computed tomography and conventional dental radiographs. Aust Orthod J. 2003; 19(2):67–75.Article
[19]Grunheid T, Kolbeck Schieck JR, Pliska BT, Ahmad M, Larson BE. Dosimetry of a cone-beam computed tomography machine compared with digital x-ray machine in orthodontic imaging. Am J Orthod Dentofacial Orthop. 2012; 141(4):436–443.Article Pubmed
[20]Lee GS, Kim JS, Seo YS, Kim JD. Effective dose from direct and indirect digital panoramic units. Imaging Sci Dent. 2013; 43(2):77–84.Article Pubmed
[21]Ludlow J. Dosimetry of 9000 3D Small FOV CBCT and Panoramic Unit, University of North Carolina School of Dentistry, Chapel Hill, NC, 2008. AAOMR Annual session. 2009.
[22]Davis AT, Safi H, Madison SM. The reduction of dose in pediatric panoramic radiography: The impact of collimator height and program selection. Dentomaxillofax Radiol 2014; 44(2):20140223.Article Pubmed
[23]Brody A, Frush D, Huda W, Brent R. Radiation risk to children from computed tomography. Pediatrics. 2007; 120(3):677–682.Article Pubmed
[24]Ludlow JB, Walker C. Assessment of phantom dosimetry and image quality of i-CAT FLX cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2013; 144(6):802–817.Article Pubmed
[25]Gijbels F, Jacobs R, Bogaerts R, Debaveye D, Verlinden S, et al. Dosimetry of digital panoramic imaging. Part I: Patient exposure. Dentomaxillofac Radiol. 2005; 34(3):145–149.Article Pubmed
[26]Lecomber AR, Downes SL, Mokhtari M, Faulkner K. Optimisation of patient doses in programmable dental panoramic radiography. Dentomaxillofac Radiol. 2000; 29(2):107–112.Article Pubmed
[27]Visser H, Rodig T, Hermann KP. Dose reductions by direct-digital cephalometric radiography. Angle Orthod. 2001; 71(3):159–163.Article Pubmed
[28]NCRP Report No. 145: New dental X-ray guidelines: Their potential impact on your dental practice. National Council on Radiation Protection and Measurements.Article
[29]Hujoel P, Hollender L, Bollen AM, Young JD, Cunha-Cruz J, et al. Thyroid shields and neck exposures in cephalometric radiography. BMC Med Imaging. 2006; 6:6.Article Pubmed
 Copyright
© 2012-2019 NobleResearch Group. All Rights Reserved
Copyright
© 2012-2019 NobleResearch Group. All Rights Reserved