



- Download PDF
- |
- Download Citation
- |
- Email a Colleague
- |
- Share:
-
- Tweet
-
Journal of Cancer Research & Therapy
Volume 1, Issue 1, March 2013, Pages 34–39
Original researchOpen Access
Economic evaluation of monoclonal antibody in the management of colorectal cancer
-
Ezat SW1,*
 ,
Natrah MS1,
Aljunid S2,
Rizal MA1,
Saperi S1,
Ismail S3,
Fuad I4 and
Azrif MA4
,
Natrah MS1,
Aljunid S2,
Rizal MA1,
Saperi S1,
Ismail S3,
Fuad I4 and
Azrif MA4
*Corresponding author: Ezat SW, Department of Community Health, Faculty of Medicine, UKM Medical Centre 56600, Kuala Lumpur, Malaysia, Tel.: +603 9145 5901; Mobile: +6019-3217-468. E-mail: sh_ezat@yahoo.com
Received 19 November 2012 Revised 1 January 2013 Accepted 9 January 2013 Published 16 January 2013
DOI: http://dx.doi.org/10.14312/2052-4994.2013-5
Copyright: © 2013 Ezat SW, et al. Published by NobleResearch Publishers. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
AbstractTop
Objective: This study aims to determine the cost of colorectal cancer (CRC) management and compare the cost effectiveness of cetuximab and bevacizumab in the management of CRC. Method: This economic evaluation study from a societal perspective involves collecting resource utilization data based on the clinical pathway of colorectal cancer management. The cost calculated includes drugs, human resources, administrative, investigations as well as capital cost. Patient’s cost was also calculated based on an interview with colorectal cancer patients. Effectiveness estimates for monoclonal antibody (cetuximab and bevacizumab) treatment were modeled from study respondents based on references from other studies. Results: Cost of treating a case of colorectal cancer in stage I is RM13,623 (RM12,467-RM14,777), stage II RM19,753 (RM16,734-RM23,520), stage III RM24,972 (RM20,291-RM29,654) and stage IV RM27, 163 (RM23, 192-RM31,133). Cost of CRC management increase with the increasing stage of the disease (Kruskal Wallis, X2=106, p<0.001). Based on estimates of 2671 new cases of CRC, the incremental cost of cetuximab is RM20, 556 480 and bevacizumab is RM7,557,953 at 50% stage III and IV as compared to the conventional chemotherapy. The incremental cost per quality adjusted life years gained for cetuximab is RM38,869 and RM14,290 for bevacizumab. Although both types of monoclonal antibody are considered cost effective (based on WHO guidelines of less than three times of GDP), bevacizumab is considered more cost effective than cetuximab. Cost effectiveness was sensitive to the percentage of late stages of CRC. Conclusions: Cost of treating late stage of CRC is high and bevacizumab are more cost effective compared to cetuximab in the management of the late stage of CRC.
Keywords: economic evaluation; cost effectiveness, colorectal cancer, monoclonal antibody
IntroductionTop
Colorectal cancer incidence is rapidly increasing in many Asian countries including Malaysia. It is the most common cancer in Malaysian males and the second most common in females after breast cancer. In the year 1998, the incidence rate of colorectal cancer in Malaysia is 11 per 100,000 population and it has increased to 14.5 per 100,000 population in 2006 [1] . Apart from the increasing incidence, the majority of patients presented at the late stage with poor prognosis [2–3]. First National Colorectal Cancer Patients Report showed that in 2008 only 2% of CRC patients were diagnosed at stage I and 3% at stage II. A study in 2005, showed that 53.9% of respondents presented at stage III and IV [3]. This is mainly due to the changes in population’s lifestyle such as increase prevalence of smoking, unhealthy diet, lack of exercise [4] and also low level of population’s awareness towards health, particularly colorectal cancer as well as absence of population based screening for colorectal cancer in Malaysia [5].
For many years, chemotherapy regimens use in Malaysia has been those with the active 5 fluorouracil (5-FU) and also levamisole. However, since the past few years the new third generation platinum compound, oxaliplatin and a semisynthetic topoisomerase inhibitor, irinotecan have been used for advanced staged colorectal cancer treatment. Introduction of a biologic agent, monoclonal antibody such as cetuximab and bevacizumab into the therapeutic landscape of metastatic CRC in which it has been used in conjunction with a chemotherapy regimen for example FOLFOX or FOLFIRI has been proven to be more effective, tailored and better tolerated treatment for advanced stage colorectal cancer in many countries. Cetuximab blocks the epidermal growth factor receptor (EGFR) and bevacizumab binds to vascular endothelial growth factor (VEGF) will suppress the cancer growth. In 60–80% of colorectal cancer cases, there is up regulation or over expression of EGFR gene and this is relevant for cetuximab. However 30–50% of these EGFR are mutated at KRAS gene and they are not responding to cetuximab. Therefore, the use of cetuximab is only for those with KRAS wild type and not mutated KRAS. Cetuximab improves median time to progression from 1.5 months to 4.1 months as well as median survival time from 6.9 months to 8.6 months as compared to conventional chemotherapy [6]. Cetuximab also offers important quality of life benefit in which less deterioration of quality of life scores as compared to conventional treatment and improvement in global health status at 8 weeks post treatment [7].
The addition of bevacizumab to FOLFOX4 has also been proven to improve survival duration from 10.8 months to 12.8 months for patients previously treated with fluoropyrimidine and irinotecan [8], 15.6 months to 20.3 months in combination with irinotecan, Fluorouracil and leucovorin (IFL) as compared to IFL and placebo while adverse effects related to the use of monoclonal antibody are manageable [9]. Monoclonal antibody has been approved to be used in the treatment of advanced colorectal cancer in many developed countries within Asia like Japan, Korea and Singapore [10]. In Malaysia, although it has been registered with National Pharmaceutical Control Bureau Ministry of Health, it is not yet listed in the Ministry of Health Drug Formulary due to the inadequacy of its evidence in effectiveness as well as cost effectiveness within the local settings. Therefore, it cannot be used in the public hospitals. In a scenario where the health care cost is rapidly escalating, evaluation of economic burden related to colorectal cancer treatment and a proper economic evaluation of this new mode of treatment in a local setting is crucial. This study aims to determine the cost of colorectal cancer management from a societal perspective and the cost effectiveness of cetuximab and bevacizumab in conjunction with conventional chemotherapy for the treatment of colorectal cancer.
MethodsTop
A cross sectional study was done from June to December 2011 in four public tertiary hospitals in the central region of Malaysia which provide surgical and oncology services. Confirmed colorectal cancer patients from out-patient clinic, wards and day care centers were universally selected regardless the stage of the disease or chemotherapy regime. The selection was based on criteria, age more than 18, confirmed diagnosis of colorectal cancer for at least six months, agree to participate and no mental illness.
The first part of the study was to establish a clinical pathway in colorectal cancer management. This is done through a focus group discussions conducted among expert involved in managing colorectal cancer patients such as surgeons, oncologist, pathologist, radiologist and nursing staff. As Malaysia may not have a standard protocol in CRC management, the pathway helped in reducing variation in clinical practice. Subsequently, based on clinical pathways which was developed, resources used were identified and provider’s cost was calculated based on activity based costing which includes cost of human resources, chemotherapy drugs which includes related investigations such as KRAS testing, procedures, administrative and radiological as well as hematological testing. Respondents’ sociodemographic and financial data were collected through face to face interview and review of medical records. European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire C-30 was used to evaluate patient’s quality of life. In costing analysis, few assumptions were made such as 60% of all CRC in Malaysia are KRAS wild type, MAB were only used for 2nd and 3rd line of treatment, no adverse effect of MAB, and life years saved on bevacizumab and cetuximab were the same.
Effectiveness estimates for monoclonal antibody were modeled from study respondents based on references from studies [7, 11–12]. Modeling was necessary due to the absence of local clinical trial data. The primary health outcome for economic analysis in this study is Life Years Saved. Therefore, the primary health economic outcome is the incremental cost per life years saved of cetuximab and bevacizumab vs conventional chemotherapy. Secondary analysis was performed using quality adjusted life years (QALYs) based on utility values which used physical function scores directly observed from study respondents and life years saved.
Effectiveness estimates
Life expectancy
Estimation of life expectancy in the conventional chemotherapy group was derived
from age specific mortality rate of CRC patients [12] based on life table generated.
Estimation of life expectancy in the monoclonal antibody treatment group was calculated
based on a study [11], in which survival benefit in cetuximab/ irinotecan is estimated
to be 0.18 years. Imputation of this value to the life expectancy of study respondents
resulted in life expectancy of CRC patients on both cetuximab and bevacizumab.
Life Years Saved (LYS)
The life expectancy of CRC on conservative chemotherapy are compared to the life
expectancy of the normal population to get the life years saved in conservative
chemotherapy group, while comparison on life expectancy in both types of treatment
(conservative and monoclonal antibody) give rise to life years saved in monoclonal
antibody group.
QALYs
Based on a formula QALYs = LYS x utility value and physical function score from
the EORTC QLQ C-30 represent the utility value for respondents in this study which
is on conventional chemotherapy alone and imputation of 8.5% increase in physical
function score in combination MAB with conventional chemotherapy group based on
study [7], QALYs of both treatment options was calculated and compared to get the
QALYs saved of each treatment option.
Resource utilization and cost data
Provider’s cost such as drug cost, procedure cost and investigations were calculated
based on the clinical pathway of CRC management while overhead cost, administrative
cost was included in in-patient hospitalization and out-patient consultation cost
based on University Kebangsaan Malaysia Medical Centre (UKMMC) clinical cost modeling
software output which is RM922 per in-patient per day and RM283 per outpatient clinic
visit. For in-patient cost, the median duration of hospitalization for each stage
based on the study respondents were multiplied by RM922 and for out-patient cost,
RM283 was multiplied by the average number of clinic visits for each stage based
on clinical pathways. Patient’s costs included are hospital/clinic fee, cost of
medications includes complementary and traditional medicines and other indirect
costs such as transportation cost, food and caregiver’s cost. Median patient cost
of RM661 was used to calculate the total cost of CRC management. The total cost
of CRC management of each stage of the disease was the sum cost of provider’s cost
(from clinical pathways, in-patient cost, out-patient cost) and patient’s cost.
Sensitivity analysis
One way sensitivity analysis were undertaken to capture the uncertainties in the
percentage of patients with stage III and IV in which monoclonal antibody should
be given.
ResultsTop
Sociodemographic profiles of respondents
A total of 160 respondents involved in the study. The majority came from Hospital
Tuanku Jaafar (33.8%), Hospital Kuala Lumpur (29.4%), UKMMC (29.3%) and Hospital
Selayang (7.5%). Male accounted for 57.5% of all respondents and female another
42.5%. The mean age of respondent is 58.47±12.04 years and the majority are
in the younger old age group which is 55–64 years (36.3%) while only 9.3% age >75
years old. The mean age by stage is stage II 66.50±9.84 years, stage III
57.76±11.78 years and stage IV 57.63±12.29 years. Statistical analysis
using ANOVA test shows that there is a significant difference in the mean age of
respondents of different stages and post hoc analysis showed these differences occurred
between stage II and stage III as well as stage II and stage IV in which mean age
is younger in stage III and stage IV as compared to stage II. Majority is in the
late stage of CRC (stage III and IV) 91.2% and 8.8% in stage II. According to ethnicity
Malays are 60.6% followed by Chinese 28.8%, Indian 10.0% and Sikh 0.6%. Most of
them educated up to secondary school (49.4%), only 6.9% never attend formal school.
Most of the respondents were no longer working (65.6%) in which 45.7% had to give
up working due to their disease, 24.8% pensioner, 14.3% full time housewife, 8.6%
never had any job, 5.8% only work when their health permits and 1% student at a
university. As expected 55.6% of respondent did not have monthly income which gives
median income of the respondents RM0 but for another 44.4% who have monthly income,
the median income is RM1700 (IQR2300). However, a majority (56.3%) has an income
between RM0-RM499, 5.6% between RM500-RM999, 8.8% between RM1000-RM1499, 8.1% between
RM1500-RM1999, 3.8% between RM2000 RM2499, 3.8% between RM2500-RM2999 and 13.8%
have an income of more than RM3000 per month.
Cost estimates
The societal cost of CRC management of different strategies is presented in Table
1. The mean cost of treating stage I CRC is RM13622, stage II RM19752, stage III
RM24972 and stage IV RM27377. This cost is higher when combination chemotherapy
which combines conventional chemo and monoclonal antibody is going to be used. The
mean cost of CRC management using cetuximab for stage III is RM53962 and RM37734
if bevacizumab is going to be used. For stage IV the cost is RM62124 with cetuximab
and RM45896 with bevacizumab.
| Stage | Mean cost (RM) | ||
| Conventional chemotherapy | Combination chemotherapy with monoclonal antibody | ||
| Cetuximab | Bevacizumab | ||
| I | 13622 |
- |
- |
| II | 19752 |
- |
- |
| III | 24972 |
53962 |
37734 |
| IV | 27163 |
62124 |
45896 |
| Mean | 21377 |
58043 |
41815 |
Economic burden of CRC management
Based on the CRC incidence rate of 14.5 per 100,000 populations [1] and the number
of at risk population in Malaysia are 18,423,700, the estimated new cases of CRC
a year is 2671 cases. Therefore, by using the percentage of cases for each stage
of a study [2] whereby 2.8 % stage I, 35.5% stage II, 40.2% stage III, 21.5% stage
IV
The economic burden of CRC management of new cases alone is estimated at RM62, 134,641 per year using conventional chemotherapy. Based on the estimated number of CRC new cases per year, estimated CRC with KRAS wild type at 60% and the percentage of CRC in stage III and IV between 50–90%, the economic burden of CRC management using monoclonal antibodies (cetuximab) is RM82, 691,021 at 50%, RM97, 990,155 at 70% and RM113, 231,246 at 90% stage III and IV. The cost of using bevacizumab at 50% stage III and IV is RM69, 692,473, RM79, 782,451 at 70% and RM89, 830,614 at 90%.
Effectiveness estimates
Based on median life expectancy, mean life years saved of respondents in this study
are 3.34±1.30 years and with a survival benefit of 0.18 years on monoclonal
antibody [11], the mean life years saved in patients on combination chemotherapy
and monoclonal antibody are 3.46±3.10 years. Therefore, secondary analysis
which calculates the QALYs saved for each treatment option showed that median QALYs
saved for conventional chemotherapy is 0.057±0.01 and 0.255±0.25 in
combination with monoclonal antibody.
Cost effectiveness analysis
Cost effectiveness analysis compared the three different treatment options which
are conventional chemotherapy, combination chemotherapy with cetuximab and combination
chemotherapy with bevacizumab. The costs considered are the total cost of managing
new cases of CRC a year. The effectiveness estimates are life years saved and QALYs.
One way sensitivity analysis was done at scenarios where different percentages of
stage III and IV of CRC which are 50%, 70% and 90% were considered. Table 2 showed
that compared to the conventional chemotherapy, combination chemotherapy with bevacizumab
at 50% of stage III and IV of CRC has the lowest cost per life years saved (LYS)
as well as cost per QALYs (RM7541 and RM8179). Cost per LYS and cost per QALYs is
higher when the percentage of stage III and IV CRC increase.
| Strategies | Total cost RM) | Total life years saved (LYS) | Cost/LYS (RM) | Total QALYs | Cos/QALYs (RM) |
| Conventional | 62,134,541.65 |
8,921.00 |
6,964.97 |
7826.03 |
7,939.47 |
| Cetuximab 50% | 82,691,021.4 |
9,241.66 |
8,947.64 |
8,520.49 |
9,704.96 |
| Cetuximab 70% | 97,990,155.36 |
9,241.66 |
10,603.09 |
8,520.49 |
11,500.53 |
| Cetuximab 90% | 113,231,246.10 |
9,241.66 |
12,252.26 |
8,520.49 |
13,289.29 |
| Bevacizumab 50% | 69,692,473.50 |
9,241.66 |
7,541.12 |
8,520.49 |
8,179.40 |
| Bevacizumab 70% | 79,782,451.56 |
9,241.66 |
8,632.91 |
8,520.49 |
9,363.59 |
| Bevacizumab 90% | 89,830,614.26 |
9,241.66 |
9,720.18 |
8,520.49 |
10,542.89 |
Incremental cost effectiveness
Based on the total cost of CRC management for new cases, analysis showed that with
the additional cost of RM7, 557,951 to treat a total number of new cases of CRC
with combination chemotherapy with bevacizumab at 50% of stage III and IV CRC and
a total of 528.86 QALYs saved as compared to the conventional chemotherapy, the
incremental cost per QALYs saved (ICER) is RM14, 290. One way sensitivity analysis
involving a proxy of cost variances revealed that cost effectiveness is sensitive
to the percentage of stage III and IV of CRC. Threshold analysis showed cost effectiveness
of combination chemotherapy with bevacizumab remains below the prespecified threshold
(3 times gross domestic product per capita) only if percentage of advanced stage
of CRC is between 50–90 percent but in combination with cetuximab is between 50–70
percent (Table 3) (Figure 1).
| Strategies | Total cost (RM) | Incremental cost (RM) | Total QALYs saved | Incremental QALYs saved | ICER |
| Conventional | 62,134,541.65 |
- |
152.25 |
- |
- |
| Cetuximab 50% | 82,691,021.4 |
20,556,479.75 |
681.11 |
528.86 |
38,869.42 |
| Bevacizumab 50% | 69,692,473.50 |
7,557,931.85 |
681.11 |
528.86 |
14,290.99 |
| Bevacizumab 70% | 79,782,451.56 |
17,647,909.91 |
681.11 |
528.86 |
33,369.72 |
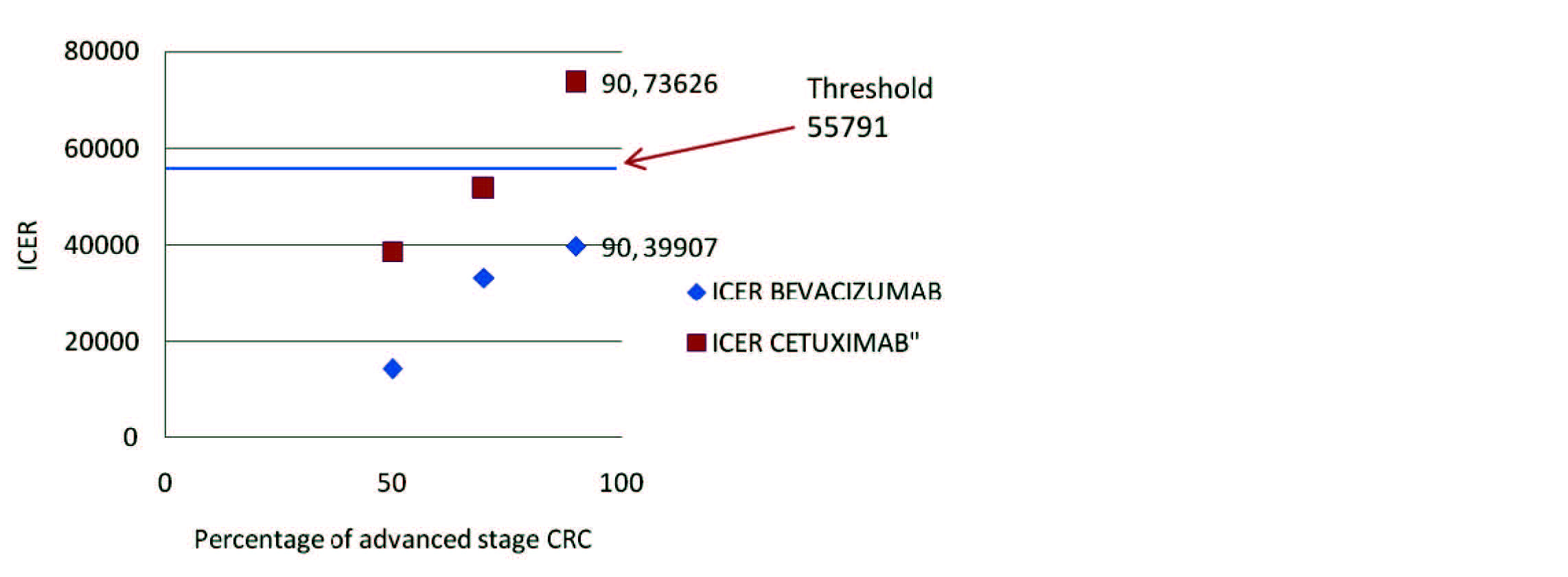
Figure 1 Cost effectiveness of combination chemotherapy with cetuximab/bevacizumab.
DiscussionTop
Combination of monoclonal antibodies with the conventional chemotherapy such as fluorouracil, oxaliplatin or irinotecan has been proven to be an effective therapeutic intervention in CRC patients who have progressed after conventional chemotherapy. Therefore, the combination of monoclonal antibodies with conventional chemotherapy is appropriate to be used as a second or third line setting. However, to introduce this new strategy for CRC treatment in Malaysian scenario requires proper clinical and cost effectiveness evidence in a local setting.
In this analysis, modeling was necessary due to the absence of local data on survival of CRC patients treated with monoclonal antibody for a direct comparison. Therefore, imputation of survival benefit of 0.18 years [11] to the respondent’s data is necessary. Although this poses some drawbacks in the result this is unavoidable because new treatment in oncology offer particular methodological problem for economic analysis as a standard comparator is absent or highly variable across treatment centers and new agent usually add new elements in the treatment pathways. Other important findings are the advanced stage of CRC are significantly higher in a younger age population (ANOVA, F=3.53, p=0.032) which reflects the lack of awareness and risky behavior among this group of population which should be addressed in health promotion activities by the authority.
The societal cost of CRC management of conventional chemotherapy in this study ranges between RM13, 622 to RM27, 163 with an average of RM21, 377. This is lower than an average cost to manage a case of lung cancer per year in Malaysia which is RM44, 725 [14]. Early stage of CRC which is stage I and II, most of the cases they only need surgical intervention whereas in lung cancer most of the cases need chemotherapy that incur a very high cost. In cervical cancer, the average cost of treatment is RM25, 623 per case per year [15].
Cost effectiveness analysis showed that the incremental cost effectiveness ratio per LYS and Incremental cost effectiveness ratio per QALY saved are higher in the combination chemotherapy with either cetuximab or bevacizumab as compared to the use of conventional chemotherapy suggesting that in general treating CRC with conventional chemotherapy is still cost effective compared to combination with monoclonal antibody. This finding is almost similar to other studies done in developed countries [12] and they conclude that the incremental cost effectiveness ratio of cetuximab over best supportive care alone is high. In Japan study also found that ICER for cetuximab plus fluorouracil/ leucovorin combination treatment was also high compared to other chemotherapies for metastatic CRC [16]. However, when we compare the six treatment option scenarios of adding a monoclonal antibody to the conventional chemotherapy alone in which the scenarios vary in the percentage of stage III and IV showed that the most cost effective option among them is the combination treatment with bevacizumab at 50% stage III and IV. This is because in Malaysia the cost of bevacizumab per cycle of treatment is lower compared to cetuximab and percentage of stage III and IV is one of the cost effectiveness drivers. Higher percentage of late stages will lower the cost effectiveness of the combination treatment (Table 2).
The incremental cost per life years saved of RM23, 569 for bevacizumab in treating CRC in this study is lower compared to other studies done in developed countries. In a UK study showed that the incremental cost per life years gained for cetuximab is about £42,975 and since their acceptable threshold is between £25,000 - £30,000, cetuximab is not considered a cost effective treatment for metastatic CRC in UK [17]. In Malaysia, since there is no threshold set as yet, therefore three times per capita gross domestic product (GDP) can be used as a guide [18]. In 2007, Malaysian per capita GDP is RM18, 597 and three times per capita GDP is RM55, 791. Based on that, combination chemotherapy with bevacizumab is a cost effective treatment provided that stage III and IV CRC are below 70% of the total cases. However, cetuximab is only cost effective when stage III and IV CRC are below 50% of the total cases. This result is not in line with other studies done in developed countries because the population sample in this study includes all stages of CRC and this caused the total cost to be lower than expected while other studies mainly done in the advanced stage CRC.
ConclusionTop
Incremental costs associated with the combination of chemotherapy with monoclonal antibody in treating CRC are high compared to the current conventional chemotherapy. Combination chemotherapy with bevacizumab is very cost effective when advanced stage CRC is below 70% and combination chemotherapy with cetuximab is cost effective only when advanced stage less than 50% of the total number of CRC patients.
Funding
This work was funded by University Kebangsaan Malaysia [FF-216–2011; UKM-DLP-2011–2029]
and Malaysian Public Health Specialist Association.
Conflicts of Interest
The authors wish to express that they have no conflict of interest
Acknowledgement
The authors would like to thank the Director General of Health, Malaysia for permission to publish this paper and Prof. Dr. Ismail Sagap, Head of Department of Surgery UKMMC, Mr. Gerald Henri, Head of Department of Surgery Selayang Hospital, Ms. Jasiah Zakaria, Head of Department of Surgery, Seremban Hospital and Mr. Zainal Rashid, Head of Department of Surgery, Kuala Lumpur Hospital for the cooperation, facilitation during data collection and all hospital directors of the four hospitals to allow the study at their facilities.
ReferencesTop
[1] National Cancer Registry: Malaysian Cancer Statistics – Data and Figure Peninsular Malaysia 2006. Ministry of Health Malaysia. Article
[2] Rashid MR, Aziz AF, Ahmad S, Shah SA, Sagap I (2006) Colorectal cancer patients in a tertiary referral centre in Malaysia: a five year follow-up review. Asian Pac J Cancer Prev 10: 1163–1166. Article Pubmed
[3] Goh KL, Quek KF, Yeo GT, Hilmi IN, Lee CK, et al. (2005) Colorectal cancer in Asians: a demographic and anatomic survey in Malaysian patients undergoing colonoscopy. Aliment Pharmacol Ther 22: 859–864. Article Pubmed
[4] Huxley RR, Ansary-Moghaddam A, Clifton P, Czernichow S, Parr CL, et al. (2009) The impact of dietary and lifestyle risk factors on risk of colorectal cancer: a quantitative overview of the epidemiological evidence. Int J Cancer 125: 171–180. Article Pubmed
[5] Kong CK, Roslani AC, Law CW, Law SC, Arumugam K (2009) Impact of socio-economic class on colorectal cancer patient outcomes in Kuala Lumpur and Kuching, Malaysia. Asian Pac J Cancer Prev 11:969–974. Article Pubmed
[6] Cunningham D, Humblet Y, Siena S, Khayat D, Bleiberg H, et al. (2004) Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med 351:337–345. Article Pubmed
[7] Au HJ, Karapetis CS, O’Callaghan CJ, Tu D, Moore MJ, et al. (2009) Health-related quality of life in patients with advanced colorectal cancer treated with cetuximab: overall and KRAS-specific results of the NCIC CTG and AGITG CO.17 Trial. J Clin Oncol 27:1822–1828. Article Pubmed
[8] Giantonio BJ, Catalano PJ, Meropol NJ, O’Dwyer PJ, Mitchell EP, et al. (2007) Bevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previously treated metastatic colorectal cancer: results from the Eastern Cooperative Oncology Group Study E3200 J Clin Oncol 25:1539–1544. Article Pubmed
[9] Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J, et al. (2004) Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 350:2335–2342. Article Pubmed
[10] Hyodo I, Suzuki H, Takahashi K, Saito Y, Tanaka S, et al. (2010) Present status and perspectives of colorectal cancer in Asia: Colorectal Cancer Working Group report in 30th Asia-Pacific Cancer Conference. Present status and perspectives of colorectal cancer in Asia: Colorectal Cancer Working Group report in 30th Asia-Pacific Cancer Conference. Jpn J Clin Oncol 40:i38–i43. Article Pubmed
[11] Starling N, Tilden D, White J, Cunningham D (2007) Cost-effectiveness analysis of cetuximab/irinotecan vs active/best supportive care for the treatment of metastatic colorectal cancer patients who have failed previous chemotherapy treatment. Br J Cancer 96:206 – 212. Article Pubmed
[12] Mittmann N, Au HJ, Tu D, O’Callaghan CJ, Isogai PK, et al. (2009) Prospective cost-effectiveness analysis of cetuximab in metastatic colorectal cancer: evaluation of National Cancer Institute of Canada Clinical Trials Group CO.17 trial. J Natl Cancer Inst. 101:1182–1192. Article Pubmed
[13] http://info.cancerresearchuk.org/cancerstats/types/bowel/ mortality.
[14] Aljunid SM, Mohd Rizal AM, Abrizah A. (2006) Cost of Smoking Among Patients with Lung Cancer. MCTC conference. Article
[15] Ezat SW, Aljunid S (2010) Comparative cost-effectiveness of HPV vaccines in the prevention of cervical cancer in Malaysia. Asian Pac J Cancer Prev 11:943–951. Article Pubmed
[16] Shiroiwa T, Fukuda T, Tsutani K (2007) Cost-effectiveness analysis of bevacizumab combined with chemotherapy for the treatment of metastatic colorectal cancer in Japan. Clin Ther 29:2256–2267. Article Pubmed
[17] NICE technology appraisal guidance 176 Cetuximab for the first-line treatment of metastatic colorectal cancer. Article
[18] Tan-Torres Edejer T, Baltussen R, Adam T, Hutubessy R, Acharya A, et al. (2003) WHO guide to cost-effectiveness analysis, World Health Organization, Geneva. Article
 Copyright
© 2012-2025 NobleResearch Group. All Rights Reserved
Copyright
© 2012-2025 NobleResearch Group. All Rights Reserved