



- Download PDF
- |
- Download Citation
- |
- Email a Colleague
- |
- Share:
-
- Tweet
-
Journal of Vaccines & Immunization
Volume 3, Issue 3, August 2015, Pages 13–18
Original researchOpen Access
Hospital epidemiology and costs of pertussis in France: A retrospective database analysis
-
Gaillat J1,*
 ,
Casez P1,
Pinquier D2,
Dommergue MA3,
Jacquard AC4,
Cancalon C5 and
Bénard S5
,
Casez P1,
Pinquier D2,
Dommergue MA3,
Jacquard AC4,
Cancalon C5 and
Bénard S5
*Corresponding author: Dr. Jacques Gaillat, Chef de Service, Infectiologie, Centre Hospitalier Annecy Genevois, France. Tel.: +33 (0)4.50636602. E-mail: jgaillat@ch-annecygenevois.fr
Received 27 March 2015 Revised 1 June 2015 Accepted 10 June 2015 Published 18 June 2015
DOI: http://dx.doi.org/10.14312/2053-1273.2015-3
Copyright: © 2015 Gaillat J, et al. Published by NobleResearch Publishers. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
AbstractTop
Background: Pertussis vaccination coverage remains unsatisfactory in adults in France and pertussis is the leading cause of death due to bacterial infection in infants up to 3 months of age, whom are most often infected by parents and siblings. The objective of this study is therefore to evaluate the epidemiologic trends in the number of cases of pertussis requiring hospitalisation and the associated costs in France between 2006 and 2012. Methods: We performed a cross-sectional, retrospective analysis of hospitalisations with a diagnosis of pertussis in France between 2006 and 2012 by means of the French diagnosis related group national program database. The initial and subsequent stays for pertussis were identified for each patient over the 7-year period. Results: A peak in the number of pertussis cases requiring hospitalisation was observed in 2009 and an even larger peak was observed in 2012. Infants under the age of 3 months had the greatest number of hospitalisations, the longest and most costly stays and the highest proportion with composite markers of severity, followed by adults aged 50 and older. Patient stays ending in death were most frequent in adults aged 50 years and older (1.4%), followed by infants under 3 months of age (0.6%), with a total of 0.6% for all ages. The mean annual crude hospitalisation rate was 1.6 per 100,000, all ages combined, and infants aged less than 3 months had a far greater 48.8 per 100,000 rate. Conclusions: This study confirms the cyclic epidemiological trends of pertussis and show two marked peaks in 2009 and 2012 of cases requiring hospitalisations in France. Infants are at the highest risk for hospitalisations and the most severe cases, followed by adults aged 50 years and older. Despite a vaccination program for infants and young parents and siblings, the burden of pertussis remains high.
Keywords: hospitalisations; pertussis; whooping cough; immunization; costs; France
IntroductionTop
Pertussis is a highly contagious bacterial disease of the lower respiratory tract whose airborne transmissibility is responsible for its spread to 80 to 90% of non-immunised close contacts [1]. The infection’s severity is primarily due to its pulmonary and neurological complications and is particularly serious in youngest infants. Adolescents and adults do not typically present with a severe form of pertussis, but it is most frequently that the house close contact, especially the parents and siblings who, as their immunity wanes, transmit the infection to infants who have not yet developed sufficient immunity [2] to be protected by immunisation program.
In France, a “cocooning” immunisation strategy around the birth has been in place since 2004 to reduce the transmission of the infection from adults to infants, wherein adults planning to have a child are recommended for a booster immunisation and close family members are recommended for a booster during the pregnancy. In addition, a booster immunisation was added to the vaccine schedule for adults at the age of 25 who have not received a dose in the previous 5 years, with a catch-up until the age of 40 [3, 4]. Despite these measures, vaccination coverage remains unsatisfactory in adults and pertussis represents the leading cause of death due to bacterial infection in infants up to 3 months of age [2, 5].
Additionally, a progressive recrudescence of pertussis has been observed and described since the early 2000’s, particularly in the United States and United Kingdom [6, 7], with increasing peaks in the number of cases every 3 to 5 years. The largest peak was described in 2011-2012. This peak was especially prominent with regard to the number of cases in infants. Besides, in France, a pertussis outbreak was described in a nursing home in 2013 (26 confirmed cases) [8].
In France, a paediatric pertussis hospital surveillance network (Renacoq) was created in 1996, but no data are available in adults. Since 1986, declaration of cases of pertussis is no longer mandatory, and there is no systematic surveillance in either the hospital or ambulatory settings. Consequently, it is difficult to evaluate the trends in pertussis infections in France.
The objective of this study is therefore to evaluate the trends in the number of cases of pertussis requiring hospitalisation in France by means of the French diagnosis related group national program database (PMSI) between 2006 and 2012. More specifically, this study aims to examine the hospital epidemiology and costs of pertussis over this 7-year period and to describe the patients presenting with these cases and their hospital stays.
Materials and methodsTop
Study design
We performed a cross-sectional, retrospective analysis of hospitalisations with a diagnosis of pertussis in mainland France between January 2006 and December 2012. The initial stay for pertussis was identified for each patient and all subsequent stays related to this disease were identified over the 7-year period. The PMSI is a national, exhaustive database that includes the characteristics of all medical and surgical stays in both public and private sector hospitals in France which uses diagnosis-related groups (DRG) for coding in order to measure hospital activity and associated costs. The PMSI uses international classification of diseases (ICD-10) and the common classification for medical acts (CCAM) codes for medical procedures.
Inclusion and exclusion criteria
Patients having at least one hospital stay in mainland France with a diagnosis (PD, RD or AD) of pertussis were included in the study. Hospital stays in the overseas departments and territories of France were excluded. The following 4 ICD-10 codes [9] were used to extract patient stays: whooping cough due to Bordetella pertussis (A370), whooping cough due to Bordetella parapertussis (A371), whooping cough due to other Bordetella species (A378) and whooping cough, unspecified species (A379). Due to the long refractory period following a natural infection by pertussis [10], the initial stay and all subsequent related stays over the 7-year period were considered to be a single case of pertussis.
Analyses
The patient’s initial stay was used for determining the socio-demographic characteristics of the case. To avoid double counting, only the date of the initial stay was taken into account in calculating the number of cases and in the epidemiologic analyses. Both the initial stay and all subsequent stays related to pertussis were included in the clinical and economic analyses of patient stays. In order to perform a subanalysis of the most severe cases of pertussis, three criteria were defined: cases requiring mechanical ventilation, cases requiring treatment in an intensive care or critical care unit (ICU/CCU) and/or cases culminating in the death of the patient [11].
Crude hospitalisation rates were determined by age group and expressed as the number of cases of pertussis requiring hospitalisation per 100,000 people in the general population. In the interest of taking different regional immunisation practices and demographic heterogeneity into account, age-adjusted hospitalisation rates were also calculated for each of 5 regions of France (Île-de-France, Northeast, Southeast, Southwest, and Northwest) and expressed in the same manner. The reference data for the general population, by age and by region, were drawn from the national institute of statistics and economic studies’ (INSEE) population estimates for the years 2006-2012 [12, 13].
The hospital perspective was used for the economic analyses. Costs of patient stays were determined by using the national common methodology cost scale (ENCC), which is published each year by the technical agency on hospital information (ATIH) for both public and private healthcare facilities. The ENCC provides a mean cost per DRG which is determined through an in-depth micro-costing analysis of a representative sample of facilities and takes into account all resources consumed for a given patient in a specific DRG. The absence of ENCC data for 2012 and for private facilities for 2008 required applying data from the previous year.
Statistical analyses were performed using SAS V9.2® software (SAS Institute Inc. Cary, NC, USA). Numbers or percents were provided for categorical variables. Mean value and standard deviation (SD) were reported for continuous variables. Results for continuous variables were compared using the Kruskall-Wallis test whereas results for categorical variables were compared using the Chi2 test or Fisher exact test when one or more cells had an expected frequency or five or less. A p value < 0.05 was considered statistically significant.
Ethics
Permission to extract and use the PMSI data was obtained from the national commission on informatics and liberty (CNIL).
ResultsTop
Patient characteristics and description of cases
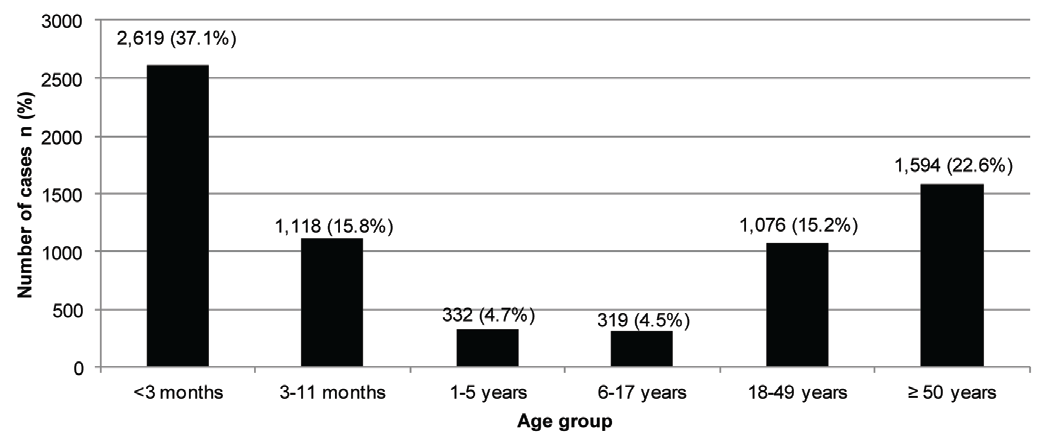
For the 2006-2012 study period, 7,058 hospitalised patients with pertussis were identified, among them 44.9% were male. More than half the patients were less than 1 year old, with the highest proportion being less than 3 months old (Figure 1). Patients aged 50 years or older represented the second largest age group and children aged between 6 and 17 years the smallest. Part of patients were infected by Bordetella pertussis (37.3%) and Bordetella parapertussis (2.0%) whereas in most cases the species of Bordetella were not specified (58.0%) or other species (2.7%). Two prominent peaks in the number of cases are visible in 2009 and 2012 (Figure 2). The greatest number of initial stays for pertussis took place in 2012.
Hospital epidemiology
No consistent seasonal variation was observed in the number of cases requiring hospitalisation in a given month over the 7-year study period. The mean crude hospitalisation rate for all age groups combined over the 7-year period was 1.6 per 100,000, but was far higher in infants under 3 months of age (48.8 per 100,000) (Table 1). There were two peaks in the mean crude hospitalisation rates, in 2009 and 2012, corresponding to the peaks in the number of cases requiring hospitalisation. These peaks in hospitalisation rates were particularly prominent for infants under 1 year of age (82.9 and 116.0 per 100,000, respectively, in 2009 and 2012). Upon adjusting the crude hospitalisation rates for age and region, no major differences in age-adjusted rates were observed and the two peaks in 2009 and 2012 were noticeable for all regions.
| Year | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | Total (2006-2012) |
| Crude hospitalisation rate (per 100,000) | p-value <0.0001 | |||||||
| <3 months | 49.3 | 32.3 | 41.9 | 58.3 | 34.6 | 45.3 | 79.7 | 48.8 |
| ≥3 and <12 months | 20.1 | 16 | 16.2 | 24.6 | 15.6 | 16.9 | 36.3 | 20.8 |
| ≥1 and <5 years | 1.0 | 0.9 | 1.0 | 1.8 | 0.9 | 1.1 | 2.0 | 1.2 |
| ≥5 and <18 years | 0.5 | 0.5 | 0.4 | 0.7 | 0.5 | 0.2 | 0.7 | 0.5 |
| ≥18 and <50 years | 0.5 | 0.5 | 0.6 | 0.8 | 0.6 | 0.5 | 0.7 | 0.6 |
| ≥ 50 years | 0.6 | 0.9 | 1.3 | 1.6 | 1.0 | 0.9 | 0.9 | 1.0 |
| Total | 1.4 | 1.2 | 1.5 | 2.1 | 1.3 | 1.4 | 2.2 | 1.6 |
| Age-adjusted hospitalisation rate (per 100,000) | p-value <0.0001 | |||||||
| Ile-de-France | 1.7 | 1.4 | 2.0 | 1.9 | 1.2 | 1.3 | 2.3 | 1.7 |
| Northeast | 1.2 | 1.3 | 1.4 | 2.0 | 1.0 | 1.1 | 2.1 | 1.4 |
| Southeast | 1.2 | 1.1 | 1.6 | 1.8 | 1.3 | 1.5 | 2.0 | 1.5 |
| Southwest | 1.3 | 1.2 | 1.6 | 3.1 | 1.9 | 1.4 | 2.6 | 1.9 |
| Northwest | 1.6 | 1.2 | 1.2 | 2.3 | 1.4 | 1.8 | 2.4 | 1.7 |
| Total cost (€) | * | * | 4,317,268 | 6,335,117 | 3,587,002 | 3,942,702 | 6,587,529 | 24,769,617 |
*Data for costs in 2006 and 2007 were not taken into account due to the DRG being revaluated in 2008.
Description of patient stays
The mean number of stays per case of pertussis during the study period was 1.12 (SD ± 0.43, 95% CI 1.11-1.13), with 90.6% of cases having a single stay, 7.5% having 2, 1.5% having 3, and 0.4% having at least 4 stays. Overall, 93.4% of stays were for at least 1 day and an overnight stay. The mean length of stay for those staying at least overnight was 7.5 ± 8.7 days, and was lengthier in infants under 3 months of age (8.8 ± 8.5 days) and adults aged 50 years or older (9.6 ± 9.0 days) (Table 2).
| Age | <3 months | 3-11 months | 1-5 years | 6-17 years | 18-49 years | ≥ 50 years | Total | p-value |
| Number of stays | 3,108 | 1,261 | 355 | 332 | 1,149 | 1,702 | 7,907 | |
| Mean (±SD) length of stay (days) | 8.8 (± 8.5) | 5.9 (± 7.7) | 3.4 (± 7.5) | 3.0 (± 4.1) | 5.2 (± 9.4) | 9.6 (± 9.0) | 7.5 (± 8.7) | <0.0001* |
| Number of stays beginning in ED (%) | 1,951 (62.8) | 783 (62.1) | 222 (62.5) | 193 (58.1) | 441 (38.4) | 721 (42.4) | 4,311 (54.5) | <0.0001 |
| Number of stays for severe cases (%) | 595 (19.1) | 95 (7.5) | 22 (6.2) | 8 (2.4) | 51 (4.4) | 150 (8.8) | 921 (11.6) | <0.0001 |
| Stays with ICU/CCU component | 12.4 | 2.4 | 2.0 | 0.6 | 2.3 | 4.6 | 6.7 | |
| Stays with mechanical ventilation | 15.0 | 6.8 | 5.6 | 2.1 | 3.1 | 5.8 | 9.0 | |
| Number of cases | 2,619 | 1,118 | 332 | 319 | 1,076 | 1,594 | 7,058 | |
| In-hospital mortality N (%) | 22 (0.8) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.1) | 25 (1.6) | 48 (0.7) | <0.0001 |
| Mean (±SD) cost per case (€) | 5,463.66 (± 4,325.15) |
4,230.28 (±3,188.96) |
3,110.03 (±2,707.13) |
2,731.99 (±1,991.64) |
3,518.93 (±4,078.15) |
4,955.30 (±3,938.05) |
4,631.43 (± 3,981.57) |
<0.0001* |
*For the variables length of stay and cost, we also tested following groups: <3 months vs 3months-49 years (p<0.0001) and <3 months vs ≥50 years (p<0.0001).
Over half of patient stays began in the emergency department (ED), and this proportion was the highest in infants under 3 months of age (62.8%). The overall percentage of stays for severe cases of pertussis was 11.6%, with infants under 3 months of age (19.1%) followed by adults aged 50 and older (8.8%). Children and adolescents aged 6-17 years and adults aged 18-49 presented the fewest severe cases (2.4% and 4.4%, respectively). Infants under 3 months of age had by far the most stays with a journey through an ICU and/or CCU (12.4%) and requiring mechanical ventilation (15.0%). On the other hand, patient stays ending in death were most frequent in adults aged 50 years and older (n=25, 1.6%), followed by infants under 3 months of age (n=22, 0.8%) and adults aged 18 to 50 years (n=1, 0.1%), with a total of 48 deaths (0.7%) for all age groups. In adults aged 50 years and older, an underlying condition was identified in 19 cases leading to death: heart failure/angina pectoris (n=8), cancer (n=6), asthma / chronic obstructive pulmonary disease (n=3) and diabetes with renal complications (n=2). For 4 cases, it concerned people with an age more than 90 years and with a poor performance status, and the 2 remaining cases had no specific comorbidity and were 68 and 76 years.
Economic analysis
Between 2008 and 2012, all stays for pertussis totalled an estimated €24.8 million, with a substantial increase in 2009 and especially in 2012 (Table 1). Costs for 2006 and 2007 were not included due to the DRG being reappraised in 2008 thereby rendering the two periods incomparable. The mean cost per stay over this 5-year period for all age groups was €4,631.43 (Table 2). The mean cost per stay was the highest for infants less than 3 months of age (€5,463.66) where the proportion of patients having an assist ventilation is higher, followed by adults aged 50 years and older (€4,955.30).
DiscussionTop
This study is, to our knowledge, the first to examine the recent epidemiological trends of pertussis cases requiring hospitalisation on the national level as well as the first to give a global picture including adults and the eldest.
The PMSI database is exhaustive at national level but was not developed for epidemiological studies. Indeed, it is a tool to measure hospital activity and to costs hospital stays according to DRG. As the rating is related to the patients’ characteristics, clinical diagnoses and procedures, the collection of data over the hospital stay is more and more accurate. A national agency (ATIH) manages this database and publishes regularly guidelines for the coding at hospital level under the supervision of a physician. For infectious diseases, the mean used for the diagnostic are not specified. But when the germ is encoded, it is assumed that a proper identification was done. This database is more and more used as a reference for epidemiological, medical and economic studies in France, even by health authorities such as Institut de Veille Sanitaire and Haute Autorité de Santé. In oncology for example, external validations were performed in comparison to existing registries, showing high sensibility and positive predictive values [14].
Previous studies on paediatric hospitalisations from the Renacoq network were published but fail to give an exhaustive picture of pertussis cases in France over the 2000-2008 period, most likely due to waning physician participation and under-reporting [15]. A peak in paediatric hospitalisations was observed in 2009, but data are limited [16]. The most recent annual incidence rate was estimated to be 210 per 100,000 in 2010 for infants under the age of 3 months [17]. Studies of the epidemiology in adults in the general practitioner setting have provided mixed results. In 1999-2000, Gilberg et al. [18] estimated the annual incidence of pertussis in the general population in the Paris area to be between 508 or 884 per 100,000. Lasserre et al. [19] found the incidence to be 145 per 100,000 among adolescents and adults in a study conducted with general practitioners, also in the Paris area. Finally, a report on nosocomial pertussis infections from 2008-2010 by the Health Surveillance Institute (InVS) concluded that the annual increase in hospital-acquired infections was greater over this period than during the 2000-2007 period, with a total of 89 cases declared between 2008 and 2010 [20].
Our results confirm the cyclic epidemiological trends of pertussis and show two marked peaks in 2009 and 2012 as also observed in other countries [6, 7]. When compared to the previously published French data cited previously, certain interesting observations can be made. Firstly, the mean annual hospitalisation rate for infants under the age of 3 months in our study was 48.8 per 100,000 over the period 2006-2012. By taking as a reference the estimated annual incidence rate of 210 per 100,000, our results show that nearly one quarter of these infants infected by pertussis are hospitalised. In the adult population, our results show that between 0.6 and 1.0 per 100,000 adults are hospitalised for pertussis, compared to between 145 and 884 cases per 100,000 in the general population. This equates to 0.06% to 0.69% of the infected adult population proceeding to be hospitalised. It can therefore be seen that pertussis is at least as common in adults as in infants, if not more so, yet only a very small percentage of infected adults develop a form of pertussis severe enough to require hospitalisation. These mirrors confirm recent findings that adults have now become the primary reservoir for the disease and are the most likely to transmit the infection to infants. Furthermore, through this indirect comparison it is seemed that infants infected by pertussis are very likely to develop a severe form, leading to hospitalisation and an increased mortality rate.
Interestingly, the small percentage of adults aged 50 years and older who did require hospitalisation was actually the population with the highest mortality rate in our study. It has to be noted that most of patients had underlying conditions. They were also the second most frequently hospitalised group after infants under the age of 3 months and were also second in terms of the most lengthy and costly stays, ahead of infants aged between 3 and 12 months. The potential severity of pertussis infections in this population has heretofore received little attention, even if a recent Australian study highlights the potential burden of pertussis among older people [20].
Rating and management of patients are different in France from other countries, so it was difficult to compare economical data to those from foreign studies [21, 22] and we did not find such data from French studies. There is a real lack of data in literature regarding cost of pertussis and it would be interesting to have further studies in near future.
Our study has several limitations. Firstly, due to the nature of the PMSI as a hospital database, this study could not evaluate the epidemiology of pertussis in the entire French population over the study period, but did evaluate the epidemiology of the cases requiring hospitalisation. Secondly, the PMSI is an administrative database primarily used to measure the activity and resource consumption of healthcare facilities, and does therefore not allow for full consideration of individual clinical cases. For example, if a stay was coded for with a diagnosis of whooping cough due to Bordetella parapertussis, it was not possible to determine if this diagnosis was determined clinically, through laboratory testing or epidemiologically. PCR is now reimbursed in France since 2011 and could increase the number of diagnosed cases. However, in our study, most of cases (58%) were encoded as undetermined, suggesting that the diagnostic is still more often based on symptoms. The spread of this technique will probably contribute to improve the diagnosis and management of this disease.
On the other hand, our study takes into account all hospitalisations for pertussis between 2006-2012, in all of mainland France and for all age groups, a scope that no other study has currently explored. Furthermore, the ICD-10 coding for pertussis remained the same during the entire study period, limiting any coding bias. Finally, we were able to retrieve all required data concerning patient stays with a diagnosis of pertussis, with very few exceptions, thereby supporting the robust nature of our analyses.
The results of this study, along with the previously reported low rates of immunisation in adults between the ages of 20 and 39 [5], suggest that the current immunisation guidelines including the “cocooning” strategy are either inadequately applied in real life or are insufficient in and of themselves in preventing the spread of pertussis to infants, as also observed recently in Canada [23]. Indeed, although the “cocooning” immunisation strategy was implemented in 2004 and a booster immunisation was added for young adults in 2008, there is no evident impact on the number of infants requiring hospitalisation. In either case, further measures are required to attempt to curb recent epidemiologic developments. Moreover, the high burden among infants aged between 3 months and 1 year suggests that there is a room of improvement for the implementation of the current vaccination strategy. The unexpected severity of cases in adults aged over 50 warrants further exploration. Additionally, further studies are necessary to determine whether or not this trend continues in the future.
ConclusionTop
This study confirms cyclic epidemiological wave with peak each three to five years. Infants under the age of 3 months represented the largest percentage of cases requiring hospitalisation. They also presented the longest stays, the most frequent use of the ED and the ICU or CCU as well as mechanical ventilation. Overall, in unvaccinated infants whooping cough remains a life threatening disease with and, nearly one-fifth of stays were considered to be for the most severe cases for infants under the age of 3 months. Surprisingly, adults aged 50 and older were the second most frequently hospitalised group and also presented longer than average stays and a higher proportion of severe cases. Mortality was highest in this population. Infants aged more than 3 months and less than 1 year are also concerned, even if a vaccination program is in place for this population. Adolescents and adults under the age of 50 represented the smallest proportion of severe cases.
Conflict of interest
Authors declare no conflict of interest.
ReferencesTop
[1]Institut National de Recherche et de Sécurité (INRS). Bordetella pertussis: agent de la coqueluche. February 2011. Accessed on 21st July 2014.Website
[2]Institut National de Prévention et d'Education pour la Santé (INPES). Guide des vaccinations: edition 2012. April 2012. Accessed on 21st July 2014.Website
[3]Haut Conseil de la Santé Publique. Calendrier des vaccinations et recommandations vaccinales 2014 selon l’avis du Haut Conseil de la Santé Publique (17–18). Accessed on 25th February 2015.Website
[4]Haut Conseil de la Santé Publique. Conduite à tenir devant un cas de Coqueluche. 2014. Accessed on 25th February 2015.Website
[5]Institut de Veille Sanitaire (InVS). Rapport d’étude sur le remboursement de vaccins contre la coqueluche chez l’adulte jeune en Île-de-France à partir des données de l’Urcam, années 2007 et 2008. July 2010. Accessed on 21st July 2014.Website
[6]Centers for Disease Control and Prevention (CDC). Pertussis (whooping cough): surveillance and reporting. March 2014. Accessed on 21st July 2014.Website
[7]Public Health England (PHE). Whooping cough (pertussis): epidemiological data. 2014. Accessed on 21st July 2014.Website
[8]Succo T, Braunstein D, Desmons S, Sampol P, Belchior E, et al. Epidémie de coqueluche dans un établissement d’hébergement pour personnes âgées dépendantes, Bouches-du-Thône, août 2013. Bull Epidémiol Hebd. 2015; (5):83-88.Article
[9]International Statistical Classification of Diseases and Related Health Problems 10th Revision. Accessed on 21st July 2014.Website
[10]Wendelboe AM, Van Rie A, Salmaso S, Englund JA. Duration of immunity against pertussis after natural infection or vaccination. Pediatr Infect Dis J. 2005; 24(5 Suppl):S58–61.Article Pubmed
[11]MedQual. La coqueluche: clinique, diagnostic et prise en charge thérapeutique. July 2013. Accessed on 21st July 2014.Website
[12]Institut National de la Statistique et des Etudes Economiques (INSEE). Population totale par âge au 1er janvier (1991-2013) par année de naissance. January 2014. Accessed on 21st July 2014.Website
[13]Institut National de la Statistique et des Etudes Economiques (INSEE). Estimation de population par région, sexe et âge quinquennal - Années 1975 à 2012. January 2014. Accessed on 21st July 2014.Article Pubmed
[14]Bossard N, Gomez F, Remontet L, Uhry Z, Olive F, Mitton N, et al. Utilisation des données du PMSI pour estimer l’incidence des cancers en France à l’échelon infranational : la démarche du groupe Oncepi. Bull Epidémiol Hebd. 2012; (5–6):77–80.
[15]Bonmarin I, Guiso N, Rosso ML, Renacoqa LP, Bruhl DL. Renacoq: surveillance de la coqueluche à l’hôpital en 2008. BEH. July 2010; 31–32.
[16]Belchior E, Bonmarin I, Poujol I, , Alleaume S, Thiolet JM, et al. Episodes de coqueluche nosocomiale, France, 2008-2010. BEH. 2011; 35–36.
[17]Belchior E. Coqueluche: données épidémiologiques et modalities diagnostiques. Presentation at the Paediatric medical-surgical societies congress, Bordeaux. June 2012.
[18]Gilberg S, Njamkepo E, Du Châtelet IP, Partouche H, Gueirard P, et al. Evidence of bordatella pertussis infection in adults presenting with persistent cough in a french area with very high whole-cell vaccine coverage. J Infect Dis. 2002; 186(3):415-419.Article Pubmed
[19]Lasserre A, Laurent E, Turbelin C, Hanslik T, Blanchon T, et al. Pertussis incidence among adolescents and adults surveyed in general practices in the Paris area, France, May 2008 to March 2009. Euro Surveill. 2011; 16(5)pii:19783.Article Pubmed
[20]Liu BC, McIntyre P, Kaldor JM, Quinn HE, Ridda I, et al. Pertussis in older adults: prospective study of risk factors and morbidity. Clin Infect Dis. 2012; 55(11):1450-1456.Article Pubmed
[21]O'Brien JA, Caro JJ. Hospitalization for pertussis: profiles and case costs by age. BMC Infect Dis. 2005; 5:57.Article Pubmed
[22]McLaughlin JM, McGinnis JJ, Tan L, Mercatanted A, Fortuna J. Estimated human and economic burden of four major adult vaccine-preventable diseases in the United States, 2013. J Prim Prev. 2015; 36(4):259-273.Article Pubmed
[23]Skowronski DM, Janjua NZ, Tsafack EP, Ouakki M, Hoang L, et al. The number needed to vaccinate to prevent infant pertussis hospitalization and death through parent cocoon immunization. Clin Infect Dis. 2012; 54(3):318-327.Article Pubmed
 Copyright
© 2012-2019 NobleResearch Group. All Rights Reserved
Copyright
© 2012-2019 NobleResearch Group. All Rights Reserved