



- Download PDF
- |
- Download Citation
- |
- Email a Colleague
- |
- Share:
-
- Tweet
-
Journal of Operative and Esthetic Dentistry
Volume 3, Issue 1, May 2019, Pages 1–5
Original researchOpen Access
Self-medication among adult patients suffering from dental pain at the Yaoundé central hospital- Cameroon
-
Ngancha Elodie Mbanya1,
Ashu Michael Agbor1,*
 , Leonard Tedong1 and
Ntungwen Charles Fokunang2
, Leonard Tedong1 and
Ntungwen Charles Fokunang2
*Corresponding author: Agbor Michael Ashu, Dentistry, Faculty of Medicine And Biomedical Sciences, Universite des Montagnes Dental School, P.O. Box 208, Bangangte, Cameroon. Tel.:+237 677170167; E-mail: agborasm@gmail.com
Received 6 March 2019 Revised 8 April 2019 Accepted 20 April 2019 Published 29 April 2019
DOI: http://dx.doi.org/10.14312/2398-029X.2019-1
Copyright: © 2019 Mbanya NE, et al. Published by NobleResearch Publishers. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
AbstractTop
Self-medication is widely practiced all over the world especially in developing countries where there is high accessibility to drugs. The aim of this study was to describe the practice of self-medication among adult patients suffering from dental pain consulting at the dental clinic of the Yaoundé Central Hospital. We conducted a cross sectional descriptive study between February to April 2018. We recruited 282 consenting respondents whom we interviewed using a structured pre-tested open ended and close ended questionnaire. Almost three quarters 208(73.8%) of the respondents admitted to had self-medicated, with a female predominance 175(62%). The most frequently used drugs were non-steroidal anti-inflammatory drugs 101(36.5%) and analgesics 94(33.2%). The most consumed analgesics and non-steroidal anti-inflammatory drugs (NSAIDs) were paracetamol 102(37%) and ibuprofen 70(25%) respectively. Reasons for self-medication were unbearable pain 108(38.5%), financial difficulties 80 (28.4%), lack of time to consult a dentist and long waiting hours at the dental office 53 (18.8%). Three quarters 201(71.2%) of the respondents practised irresponsible self-medication and 81(28.9%) practiced responsible self-medication. The sources of medications included pharmacy 127(45.2%) and non-pharmaceutical establishments such as previously prescribed medications at home 109(38.5%), roadside vendors 31(11.1%), open markets 10(3.8%) and mobile vendors in buses or transport cars 4(1.4%). Less than three quarters of the respondents 73(26%) who were aware of complications of self medications such as gastric ulcers, drug resistance, allergies and overdose. Self-medication remains a rampant practice in our community. There is need to enforce formulate policies that can limit self-medication practices in the community.
Keywords: self-medication; dental pain; drugs; Yaoundé
IntroductionTop
Enamel caries starts as a symptomless lesion as a result of destruction of the hard tissues of the tooth. When the destruction of dental hard tissues gets to the dentine, the patient start feeling mild pain or dental sensitivity. The intensity of the pain depends on the dept of tooth destruction or cavity towards the pulp chamber. This pain may become unbearable when it gets to the pulp chamber (which contain the neurovascular tissues) of the teeth. Anxiety due to a phobia for dentists and their practice and toothache are the most likely symptoms that may warrant patients to embark on self-medication [1].
The use of medications without prior medical consultation regarding indication, dosage, and duration of treatment is referred to as self-medication [1]. Though rampant throughout the world, it is becoming a very serious problem in developing countries as individuals obtain and consume self-prescribed drugs without seeking medical advice. The prevalence of self-medication has been estimated to be 10.3% and 87% worldwide. This vary according to the socio economic status of the population, the type of disease and method of drug use [2].
Drugs mostly used to self-medicate are called non-prescription or over-the-counter (OTC) drugs. Apart from over the counter medications, some patients use prescribed medicines as well as alternative medicines such as food supplements, herbal remedies and traditional products to self-medicate. As such the inappropriate use of these medicines exposes patients to dangers such as overdose, adverse drug reaction, undesirable side effects, drug dependence and microbial resistance. The danger most of the time is that many who self-medicate are unaware of these consequences [3].
Though many dentists are aware that many patients self-medicate as a result of dental pain, recent studies have shown that as much as 70% of all patients with dental pain still complain after self-medicating with analgesics [4-6]. This signifies that most medicines used for self-medication do not treat the illness but only provide symptomatic relief. Therefore the best therapy for dental pain is to treat the root cause which requires an accurate diagnosis for proper treatment [4].
A study carried out in a rural area in Cameroon on self-medication as a result of tooth ache showed that 64.5% of the respondents used pharmaceutical products while 7.7% used dangerous substances such as petrol and vinegar for self-medication. There is paucity of literature on the frequency of self-medication in urban areas in Cameroon. The objective of our study was to determine the frequency and reasons of self-medication amongst adult patients suffering from dental pain attending the Yaoundé Central Hospital.
MethodologyTop
This was a descriptive cross sectional study carried out on patients who suffered from dental pain and attended the dental department of Yaoundé Central Hospital between February to April 2018.
Selected in this study were all adult patients who presented with dental pain consulting for their first time at the dental department in Yaoundé Central Hospital were selected using convenient sampling. A structured pre-tested open ended and closed ended questionnaire was used to collect data from the patients. The questionnaire was used to collect information on the socio-demographic status of respondents, presenting complain, duration of self-medication, reasons for resorting to self-medication, drug(s) used for self-medication, source of the drug(s), type of self-medication, the posology (dose taken) determined, knowledge about the side effects of drug(s) used, awareness of the consequences of self-medication.
Data was collected in Microsoft excel 2010 and analysed data using Statistical Package for Social Sciences (SPSS) version 20. Data were presented as frequencies, percentages, mean, and standard deviations. Comparative statistics was done using Fisher's exact test, and P < 0.05 was considered as significant.
Ethical considerations
Ethical clearances were taken from the Institutional Ethics Committee (IEC) of Université des Montagnes and the Yaoundé Central Hospital. Written informed consent was taken from each participant.
ResultsTop
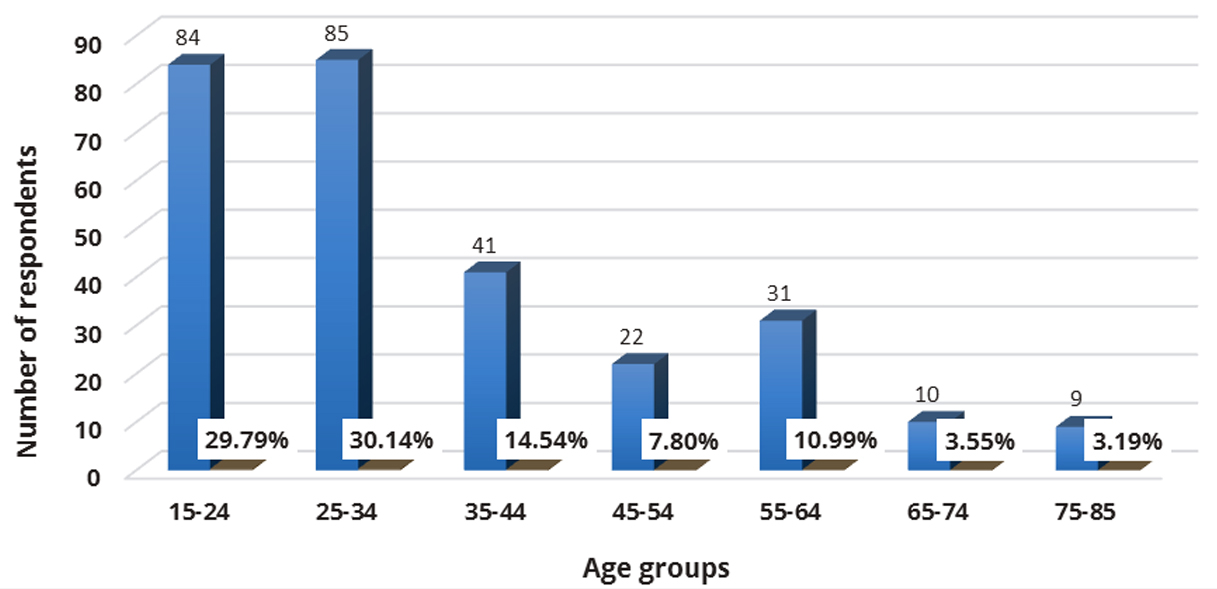
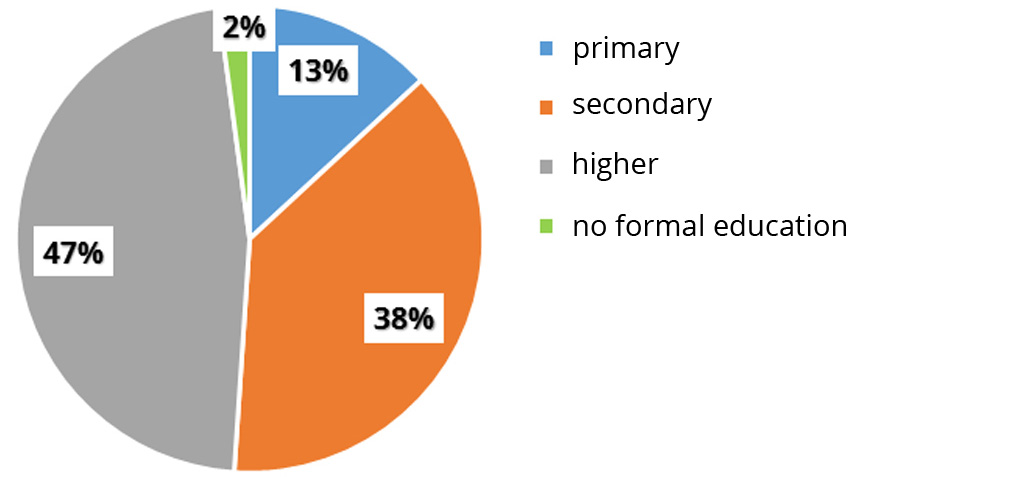
Out of the 282 patients who presented with dental pain, 208 had self-medicated. The age of the patients varied between 15 to 85 years. This included 46% of workers, 40% of students, 12% unemployed and 2% retired. There was a female 128(62%) predominance in the practice of self-medication compared to male 80(38%). A third 85(30.14%) of the self-medicated patients were within the 25 to 34 years age range, closely followed by the 15 to 24 years age group representing 84(29.79%) patients. The mean age was 35.7±16.4years (Figure 1). Less than half 132(47%) of the respondents had attained higher level of education and a third 107(38%) secondary level of education (Figure 2).
Reasons for self-medication
More than a third 80(38.5%) of the patients self-medicated because of pain, 59(28.4%) because of financial difficulties and 39(18.8%) because of lack of time to consult a dentist (Table 1).
| Respondent | Number of respondents | Percentage (%) |
| Unbearable pain | 80 | 38.5 |
| Financial difficulties | 59 | 28.4 |
| Lack of time | 39 | 18.8 |
| Dental phobia | 21 | 10 |
| Advice from family | 6 | 2.9 |
| Others | 3 | 1.4 |
| Total | 208 | 100 |
Drugs used by patients for self-medication
More than a third 112(36.5%) of the patients self-medicated with non-steroidal anti-inflammatory drugs, a third 102(33.2%) with analgesics, 54(17.6%) with antibiotics and 27(8.8%) traditional medicines (herbs such as thyme and cloves, mango bark) by were equally used. Other substances consumed by patients included food spices, alcohol and vinegar (Table 2).
| Drug class | Number of respondents | Percentage (%) |
| Non-steroidal anti-inflammatory drugs (NSAIDs) | 112 | 36.5 |
| Analgesics | 102 | 33.2 |
| Antibiotics | 54 | 17.6 |
| Traditional medicine | 27 | 8.8 |
| Mouthwash | 6 | 2 |
| Others | 6 | 2 |
Drugs used and sources of drugs procurement used for self-medication
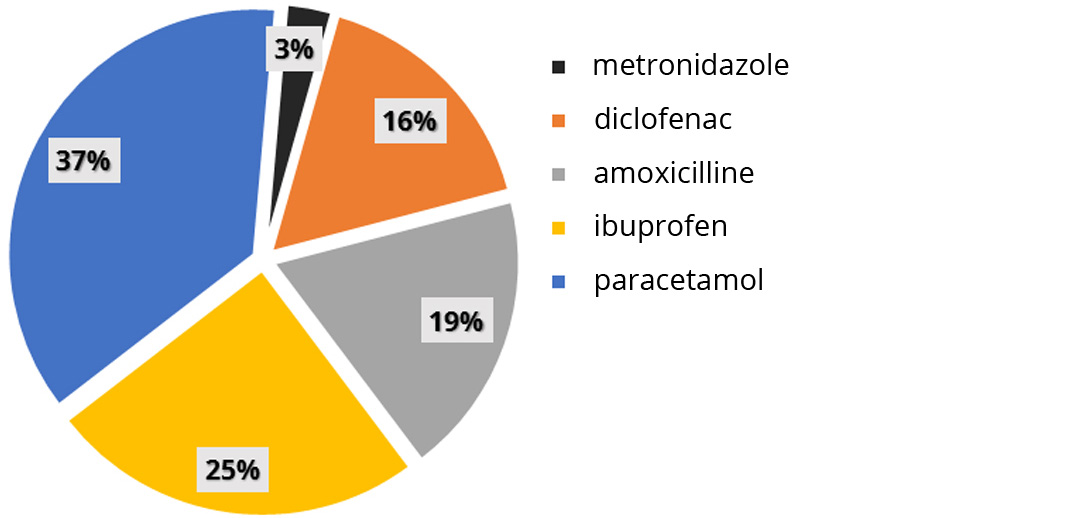
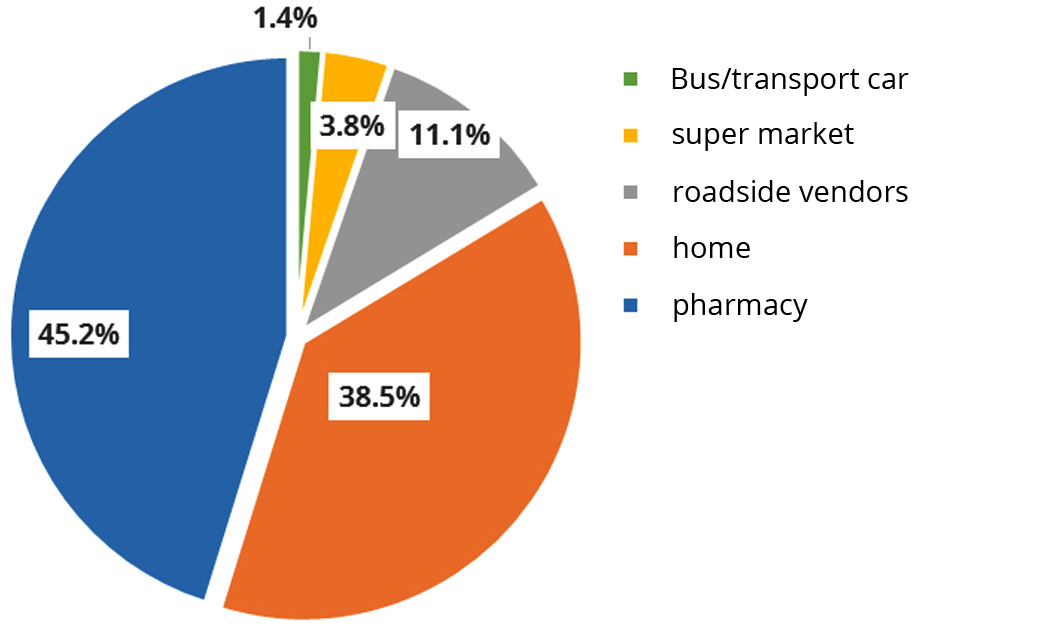
More than a third 98(37%) self-medicated with paracetamol, 66(25%) ibuprofen and 50(19%) amoxicillin (Figure 3). Almost half 94(45.2%) obtained their drug from pharmaceutical establishments meanwhile, 80(38.5%) used drugs from their first aid box at home and 23(11.1%) got the drugs from roadside vendors (Figure 4).
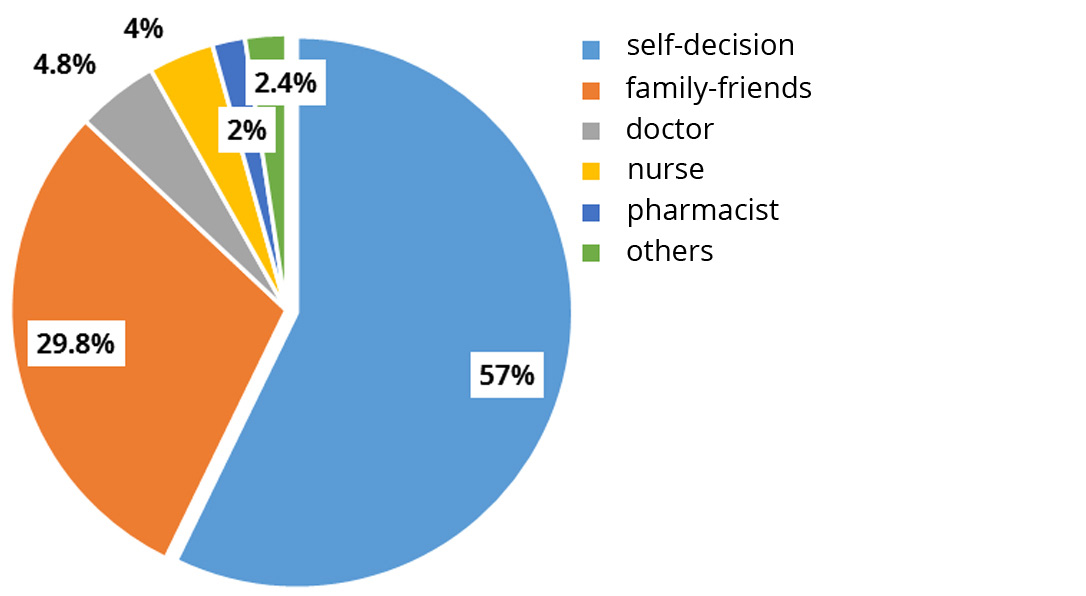
Sources of drug information used in self-medication
More than half 119(57%) self-medicated voluntarily without any advice, 62(29.8%) from advice of family and friends, 10(4.8%) advice from a non-certified medical personnel were 8(4%) from a nurse and 4(2%) from a pharmacist. The other source mentioned by a few was roadside vendor and the internet (Figure 5).
Determination of drug dosage when self-medicating
The posology (Drug dosage) was determined mostly by the consumers themselves 49(23.6%), 41(19.7%) by a pharmacists, 41(19.7%) family and friends, 23(11%) read the drug leaflet, 17(8.2%) received advice from the drug vendor, 15(7.2%) from old prescriptions from previous dental consultations and 12(5.8%) got advice from a doctor (Table 3).
| Ways by which drug dosage were determined | Number of respondents | Percentage (%) |
| Instinct | 49 | 23.6 |
| Pharmacist | 41 | 19.7 |
| Family-friends | 41 | 19.7 |
| Drug leaflet | 23 | 11 |
| Drug vendor | 17 | 8.2 |
| Old prescription | 15 | 7.2 |
| Doctor | 12 | 5.8 |
| Nurse | 7 | 3.4 |
| Internet | 3 | 1.4 |
Patient`s awareness on the risks in self-medication practice
Three quarters 154(74%) of the patients were not aware of the dangers of self-medication, 54(26%) of the patients cited microbial resistances, 3(5.6%) allergies, 6(11.5%) dizziness 8(15%), gastric ulcers 12(22.2%) and drug overdose 26(48.2%).
Patients and their self-medicated drugs sources
Among patients who self-medicated, 40(19.2%) males and 54(26%) females got their drugs from pharmaceutical establishments meanwhile 40(19.2%) males and 74(35.6%) females got their drugs from non-pharmaceutical establishments (Table 4).
| Gender/ Profession | N (%) | P value |
| Non-phamaceutical - Gender | ||
| Female | 73(25.9) | 0.023 |
| Male | 40(14.2) | 0.0157 |
| Pharmaceutical - Gender | ||
| Female | 55(19.5) | 0.008 |
| Male | 40(14.2) | 0.0109 |
| Grand total | 208(100) | |
| Non-phamaceutical - Profession | ||
| Not working | 62(21.9) | 0.048 |
| White-collar worker | 27(9.6) | 0.121 |
| Blue-collar worker | 24(8.5) | 0.145 |
| Pharmaceutical - Profession | ||
| Not working | 45(15.9) | 0.061 |
| White-collar worker | 24(8.5) | 0.072 |
| Blue-collar worker | 26(9.2) | 0.089 |
| Grand total | 208 | |
DiscussionTop
Pain, discomfort or emotional distress has a number of ways of influencing the health seeking behaviours because of the urgent need for palliation for their immediate discomfort. In developed countries, strict pharmacovigilance law has kept the frequency of self-medication at a low level accounting for around 5% to 10% of drugs sales [7]. In the current study, three quarters of respondents self-medicated. This is relatively high and this results is similar to that of Anyanechi et al., in an urban setting in Nigeria [8]. This high frequency of self-medication might be as a result of easy access to OTC medication and poor access to oral health care facilities. Agbor and Azodo, reported a high frequency of self-medication in an earlier study carried out in Cameroon and the major reasons for this was easy access to non-prescribed medications [5].
The female predominance in the current study could be due to dental phobia and low pain threshold in women. Though women have a better health seeking behaviour than males, their regular hospital visit may influence their familiarity with the drugs, thus making them to self-medicate more [3, 8].
In the current study, the 25-34 years age group was more represented. This falls within the active age group of busy individuals who do not have time to consult in a dental clinic and will rather prefer to self-medicate before consulting when the pain is severe. This could also be explained by the fact that the main cause of dental pain amongst young adults was caries due to snacking and cariogenic diets. These results are similar to those obtained by Azodo and Ololo, with 21-30 years and Anyanechi et al., and with 28-37 years [8, 9].
Reasons for self-medication
A third of the respondents self-medicated because of pain. This was previously reported in other studies by Souaga et al., Azodo and Ololo, and Anyanechi et al. [7-9]. It has been reported that most patients seek dental help only when pain becomes unbearable and that in most cases, no relieve is experienced after self-medicating [5, 7].
The second reason revealed by patients was financial difficulties, the cost of dental treatment according to these patients was relatively high, prompting them to self-medicate [5, 7]. Agbor and Azodo obtained similar results [5, 7].
Another aspect was lack of time where patients complained about long waiting hours at the dental office. Also being busy with their daily activities, they preferred to self-medicate while waiting to schedule a time for consultation. A similar result was obtained in a study by Anyanechi et al., who showed that 18.7% self-medicated due to time constraints [7]. Similar results were reported by Agbor and Azodo, and Souaga et al., [5, 9]. Dentophobia 10% who revealed being afraid of the dentist and came to consult only due to pain constraints. Some patients believed that the major treatment at the dental office is tooth extraction, which they feared and thus preferred to self-medicate. This was shown in a study by Souaga et al. (11.54%) in Ivory coast [9].
Drugs used for self-medication
The medications most commonly used by the patients in our study was non-steroidal anti-inflammatory drugs, antipyretic analgesics and antibiotics used either singly or in combination. More than a third of the respondent consumed paracetamol, followed by ibuprofen and amoxicillin. This result is similar to that of souaga et al., [9] and Anyanechi et al., [7]. This could be explained by the fact that these drugs are easily accessible both in pharmaceutical and non-pharmaceutical establishments and these patients presented pain complaints. In contrast, Azodo and Ololo’s, findings revealed that analgesics were the most used drug by followed by antibiotics i.e., amoxicillin and tetracycline by 39(17.1%) and 9(3.9%) respectively. But in this same study no anti-inflammatory drugs were used [8]. This could still be due to the differences in social habits and the study population. Traditional medicines were used by a minority in our study contrary to the findings by Agbor and Azodo, in Cameroon and that of Simon et al., in India who revealed that traditional medicines were the second most used drug [5, 11]. This difference may result in fact that our study was hospital based while the previous study was population based.
Type of self-medication practiced
We found that almost half of the patients bought their drugs in a pharmacy and this result is lower than 64.5% found by Agbor and Azodo in Cameroon, 86.5% found by Giriraju in India [3, 5]. Most patients were not covered by insurance for their health issues and medications needed and thus not being able to pay for their drugs in pharmacies because they are affordable in non-pharmaceutical establishments. Some had drugs in their pharmacy (First aid) cupboards at home and thus self-medicated when need be, while others (16.3%) got them from roadside vendors, markets and bus/ transport cars. Similarly, Souaga et al., in Ivory coast showed that 14.10% of their study population bought drugs in the streets or market places whereas Agbor and Azodo obtained 26.1% for roadside vendors and 5.3% for street vendors. This reveals that there is a high rate of roadside drug purchase and this is dangerous because these drugs might not be authentic or expired. There is need for law reinforcement and serious control as concerns the sales of drugs in our community. No patient in our study got their drugs from native healers contrary to other studies [5, 9]. The patients who consumed traditional medicines (herbs such as thyme and cloves, mango bark) had them at home or got them from a relative.
More than half of the respondent in our study who self-medicated depended on personal knowledge to self-medicate and determined the doses from family and friends, drug leaflets, old prescriptions and researched on internet. The others had the dose of their self-medicated drugs determined by drug vendors. This is confirmed by the fact that three quarters of the respondents practiced irresponsible self-medication as they didn’t get advice from a health professional. several other studies have revealed that patients got advice from, leaflets, relatives and friends [3, 8, 12]. A minority however got their information from health professionals including pharmacists, medical doctors and by nurses.
In the current study, less than a third of the patients who self-medicated were ignorant on the adverse effects of the medications they were taking. This is alarming because certain drugs such as antibiotics when used irrationally, can lead to antimicrobial resistance, addiction, hepatotoxicity and gastro-intestinal complications [11, 14].
ConclusionTop
Self-medication is highly practiced amongst adult and adolescence patients with toothache. In our study, the frequency of self-medication was very high was more common among women and people between the ages of 25 to 34-years-old. The main reasons for self-medication were; to relieve unbearable pain, financial difficulties and lack of time to consult a dental clinic. The type of drugs most frequently used were non-steroidal anti-inflammatory drugs, analgesics and antibiotics. Paracetamol, ibuprofen and amoxicillin were the most consumed medications. Irresponsible self-medication was mostly practiced and few patients who self-medicated knew about the adverse effects of this practice. Drug control policy needs to be intensified in the community and health professionals should prioritize educating the patients on proper health oral care.
Recommendations
Pharmacists should not be focused only on selling drugs but to take some time to advice and educate the patients on proper health care. Dental surgeons should educate patients on oral health, the dangers of self-medication and the proper use of over-the-counter drugs and organize oral health outreaches which will promote oral health care by educating patients on early consultations and routine dental check-ups.
Conflicts of interest
Authors declare no conflicts of interest.
ReferencesTop
[1]World Health Organization (WHO). The role of the pharmacist in self-care and self-medication: Report of the 4th WHO consultative group on the role of the pharmacist in health care system 1998.
[2]Albatti TH, Alawwad S, Aldueb R, Alhoqail R, Almutairi R. The self-medication use among adolescents aged between 13-18 years old; prevalence and behaviour, Riyadh-Kingdom of Saudi Arabia, from 2014-2015. Int J Paediatric Adolescent Med. 2017; 4:19–25.Article Pubmed
[3]Giriraju A. Perception about self-medication practices for oral health problems among the general population of Davangere city, Karnataka, India. J Indian Assoc Public Health Dent. 2014; 12(3):219.Article
[4]Rawlani SM, Rawlani S, Bhowte R, Degwekar S, Rawlani S, et al. Prevalence of self-medication among dental patients in rural area of Maharashtra, India: A cross-sectional study. Indian J Oral Sci. 2015; 6(2):51.Article
[5]Agbor MA, Azodo CC. Self-medication for oral health problems in Cameroon. Int Dent J. 2011; 61(4):204–209.Article Pubmed
[6]Baños JE, Bosch F, Toranzo I. Self-medication with analgesics. A study on odontalgia. Med Clin (Barc). 1991; 96(7):248–251.Pubmed
[7]Montastruc JL, Bagheri H, Geraud T, Lapeyre-Mestre M. Pharmacovigilance of self-medication. Therapie. 1997; 52(2):105–110.Pubmed
[8]Anyanechi C, Saheeb B. Toothache and self-medication practices: A study of patients attending a niger delta tertiary hospital in Nigeria. Ann Med Health Sci Res. 2014; 4(6):884–888.Pubmed
[9]Azodo CC, Ololo O. Toothache among dental patients attending a Nigerian secondary healthcare setting. Stomatologija. 2013; 15(4):135–140.Article Pubmed
[10]Souaga K, Adou A, Amantchi D, Kouame P, Angoh Y. Self-medication during orodental diseases in urban Ivory Coast. Results of a study in the region of Abidjan. Odonto-Stomatol Trop Trop Dent J. 2000; 23(90):29–34.
[11]Jain A, Bhaskar DJ, Gupta D, Agali C, Yadav P, et al. Practice of self-medication for dental problems in Uttar Pradesh, India. Oral Health Prev Dent. 2015; 30(1):5–11.Article Pubmed
[12]Simon A, Rao A, Rajesh G, Shenoy R, Pai MH. Trends in self-medication for dental conditions among patients attending oral health outreach programs in coastal Karnataka, India. Indian J Pharmacol. 2015; 47(5):524–529.Article Pubmed
[13]Harshvardhan C, Kaushal S. Self-medication practices in dental patients in rural Gujarat, India. IJOCR. 2015; 3(4):15–20.Article
[14]Vidyavati SD, Sneha A, Kamarudin J, Katti SM. Self-medication - reasons, risks and benefits. Int J Healthc Biomed Res. 2016; 4(4):21–24.Article
 Copyright
© 2012-2025 NobleResearch Group. All Rights Reserved
Copyright
© 2012-2025 NobleResearch Group. All Rights Reserved