



- Download PDF
- |
- Download Citation
- |
- Email a Colleague
- |
- Share:
-
- Tweet
-
Journal of Radiology and Imaging
Volume 1, Issue 1, July 2016, Pages 1–5
Original researchOpen Access
Clinical evaluation of near-infrared light transillumination (NIRT) as an interproximal caries detection tool in a large sample of patients in a private practice
-
Francesco Russotto1,
Federico Tirone1,*
 ,
Stefano Salzano1,
Francesco Coero Borga1,*,
Davide Paolino2,
Alberto Ferraro1 and
Samanta Botasso3
,
Stefano Salzano1,
Francesco Coero Borga1,*,
Davide Paolino2,
Alberto Ferraro1 and
Samanta Botasso3
*Corresponding author: Dr. Federico Tirone, DDS., Clinica Odontoiatrica Salzano Tirone, Via Cascina Colombaro 37, 12100 Cuneo, Italy. Tel.: +390171619210; Fax: +3901711890124; E-mail: federico.tirone@gmail.com. Dr. Coero Borga FA, Department of Mechanical and Aerospace Engineering, Politecnico of Turin, Turin, Italy. E-mail: francobor@libero.it
Received 8 April 2016 Revised 2 June 2016 Accepted 17 June 2016 Published 24 June 2016
DOI: http://dx.doi.org/10.14312/2399-8172.2016-1
Copyright: © 2016 Russotto F, et al. Published by NobleResearch Publishers. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
AbstractTop
Background: A study has been carried out in order to evaluate in vivo the diagnostic performance of near-infrared light transillumination (NIRT) compared to digital radiographic examination (RE) in the detection of class II carious lesions. Methods: A total of 114 patients were included, and 2957 proximal surfaces were considered. Surfaces were imaged by means of NIRT and radiographed with a photostimulable phosphor system. NIRT and radiographic images were observed by two blinded operators. Their diagnoses were compared with those made while visiting the patients, when visual-tactile, radiographic and NIRT data were matched by expert operators to obtain the reference diagnoses. Sensitivity, specificity and inter-observer consistency were calculated. Results: Throughout the visits, 395 caries were detected. When investigating without clinical information and in a blind manner, RE performed significantly better than NIRT regarding sensitivity analysis (0.591 vs. 0.456, p<0.001), and NIRT performed significantly better than RE regarding specificity analysis (0.980 vs 0.933, p<0.001). However, NIRT showed sensitivity similar to RE when only enamel caries were concerned. With regard to the agreement between the two observers, NIRT performed significantly better than RE (0.901 for RE analysis, 0.989 for NIRT analysis, P<0.001). A high probability of false positives for enamel caries (95% from 0.699 to 0.791) was observed in RE. NIRT was very likely to detect and correct the erroneous positive diagnosis of enamel carious lesions obtained using RE (95% CI for probability from 0.938 to 0.979). Conclusions: NIRT should be used in caries diagnosis in combination with radiographic images. In fact, NIRT can help to correct a false positive diagnosis of enamel caries. Furthermore, NIRT could be used to detect caries in patients for whom non-urgent radiographic exposition is contraindicated and to monitor enamel caries in medically treated patients. Finally, thanks to its three-dimensional images, NIRT can aid in detecting small caries when performing minorly invasive restorative procedures.
Keywords: clinical evaluation; near-infrared light transillumination; NIRT; radiographic examination
IntroductionTop
Currently, carious lesions should be treated with respect to dental tissue conservation. In cases of carious lesions confined to the enamel, current evidence suggests the promotion of remineralization instead of restoration [1-3]. Therefore, the early detection of enamel caries has now become mandatory. It is scientifically accepted that a correct diagnosis of interproximal caries lesions is difficult to perform for the simple fact that the lesion cannot be directly observed.
In conjunction with visual-tactile examination, either conventional or digital radiographic examination (RE) is the most commonly used method to detect and diagnose carious lesions in proximal and occlusal surfaces. The carious process results in tooth demineralization and leads to the typical radiographic appearance of caries as a radiolucent area. However, because tooth decalcification ranging from 40% to 60% is required to allow this radiographic finding, this method has shown a rather high sensitivity for the detection of dentin caries on proximal surfaces but a limited effectiveness in the detection of early lesions in enamel [4]. Further weaknesses of traditional radiography are the patient’s exposure to X-rays (in order to monitor the spreading and the progression of new lesions) and the underestimation of the real size of lesions [5].
Digital radiography, which is widely used by dental practitioners, is unable to overcome such limitations, namely, the detection of early lesions and patient exposure to ionizing radiation [6].
As a consequence, alternative methods to enhance caries diagnosis have been developed recently. Fibre optical transillumination (FOTI) and digital fibre optical transillumination (DIFOTI) use transillumination in order to detect areas of enamel or dentin demineralization, which are known to scatter more light than healthy dental tissues [7-10].
More recently, a near-infrared transillumination (NIRT) device has been introduced (DIAGNOcam®, Kavo®, Biberach, Germany). It consists of a camera for NIR light emission connected with a USB port to a computer and specific software.
Optical fibres transmit the light through the gum and alveolar bone to the dental root and then up to the crown. In cases of a carious lesions, the light is scattered and reduced via a mechanism similar to FOTI and DIFOTI but within a different light range (700 to 1500 nm), resulting in deeper tissue penetration [11, 13].
The aim of this in vivo, double-blinded study was to evaluate the diagnostic accuracy of NIR transillumination compared to digital radiography (bitewings) in the detection of interproximal caries without any clinical information or examination.
Materials and methodsTop
The study was carried out between January 2014 and March 2014 in an Italian private practice (in Cuneo).
All consecutive, unrelated adult patients who came to our practice for a first visit were considered eligible. The inclusion criterion was the existence of at least one quadrant with two premolars, and at least the first molar must not meet the following exclusion criteria: mesio-occluso-distal composite or amalgam restoration, full crown restoration, diastema, or rotated teeth. Patients who disagreed with the data collection procedures were also excluded. All patients were thoroughly informed about the diagnostic process, and a valid informed consent had to be signed before the visit in accordance with the Helsinki declaration.
All examinations were performed by two dentists with more than 10 years of experience in diagnostic practice (FT and SS).
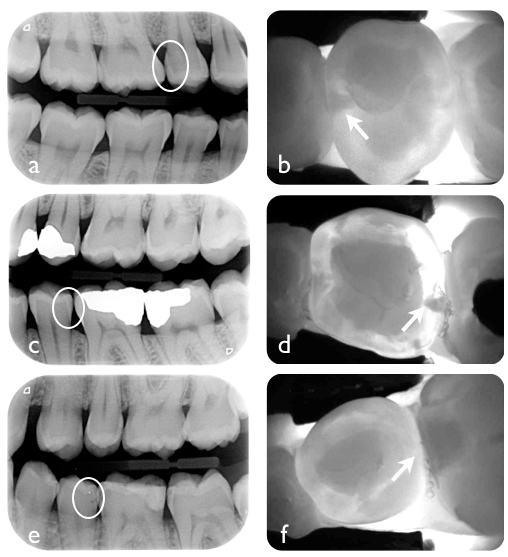
Each patient was examined with a dental mirror, a probe, a compressed air source and the LED light source of the dental unit. During the visit, a visual-tactile evaluation of carious lesions was performed, and clinical diagnosis was registered by a trained assistant. After clinical evaluation, images from all teeth were captured with a diagnostic device using NIRT (DIAGNOcam®, Kavo®, Biberach, Germany) (Figure 1); the optimal placement of the handpiece while taking the image was verified through the live image projection on a screen positioned in front of the dental unit. At least two bitewing radiographs were taken with a photostimulable phosphor system (3×4-cm plates, 7 mA, 0.16 s, 70 Kv; Vistascan® Durr dental®, Bietigheim-Bissigen, Germany) (Figure 1).
Clinical evaluation was matched with NIRT and RE data to obtain an immediate diagnosis (general evaluation) and a therapeutic plan was prepared and illustrated to the patient. Caries detected in the final diagnosis were registered by the assistant. The diagnosis made during the visit by means of visual-tactile, RE and NIRT examinations were considered to be the diagnosis of reference in this study.
Data from clinical evaluation, general evaluation, NIRT images and radiographic images were saved in different file folders. Radiographic images were labelled with patients’ initials and ordered alphabetically. NIRT images were labelled with progressive numbers.
Before the beginning of data collection, data from 10 patients were collected in the same way. These data were used to evaluate the inter-observer agreement after a two-hour calibration session.
Because the correlation was deemed to be good (see results), file folders containing the images were given to two operators with less than three years of experience in diagnostic practice (FR and AF). They could not match the data from the two folders. All images where examined, and a diagnosis of caries was made for both RE and NIRT images. Detected caries were classified according to their depth (Table 1) [14]. In fact, although a classification based on cavitation status could be a better indicator for restorative needs [15] than lesion depth, cavitation is not always easy to assess in interproximal lesions. As a result, the lesion’s progression into the dentin has become the main criterion for making operative decisions [16].
| E1 | outer 1/2 of enamel |
| E2 | inner 1/2 of enamel |
| D1 | outer 1/3 of dentin |
| D2 | middle 1/3 of dentin |
| D3 | inner 1/3 of dentin |
A descriptive statistical analysis was made to compare the diagnosis obtained with RE images alone with that obtained with NIRT images alone and with complete clinical and imaging-supported evaluation. Sensitivity and specificity for NIRT and RE in dental caries diagnoses were calculated in comparison to the diagnoses made by an experienced operator using all available tools during a clinical examination.
Performance of NIRT in comparison to RE has been calculated with a score test for binomial proportions. Inter-observer consistency was evaluated for both NIRT and radiographic evaluation. Sensitivity and consistency among operators were calculated by referring to the total caries amount and by dividing positives into groups (E1, E2, D1-D2).
ResultsTop
In the preliminary evaluation, the consistency between the two observers was 0.861 for RE and 0.936 for NIRT. A total of 276 consecutive unrelated adult patients who came to our practice for a first visit were considered: 130 of them were males (47.1%), and the average age was 44 (SD 16.3). 161 were excluded because they did not meet the inclusion criteria, and one patient had to be excluded because the NIRT device was not available during the visit. In short, 114 patients were included in this study (41.3% of the total), and 58 were males (50.9%), with an average age of 32.5 (SD 12.1). A total of 1555 teeth of the selected patients were considered, yielding a total of 2957 interproximal surfaces (Table 2).
| Overall patients considered | 276 | |
| Overall recruited patients | 114 | |
| Overall dental elements recruited | 1555 | |
| Overall interproximal surfaces recruited | 2957 | |
| Overall interproximal caries detected | 391 | |
| E1 detected caries | 143 | |
| E2 detected caries | 128 | |
| D1 detected caries | 104 | |
| D2 detected caries | 12 | |
| D3 detected caries | 4 | |
During the general evaluation, 395 caries were detected, as summarized in Table 2. The blind diagnosis distribution between the two operators is summarized in Table 3. RE sensitivity to caries detection without clinical evaluation by less-experienced operators was 0.699 for observer A.F. and 0.484 for observer R.F. NIRT sensitivity was 0.504 and 0.408, respectively. RE sensitivity was higher than NIRT sensitivity, regardless of the operator (p<0.001 for A.F, p=0.029 for F.R.) (Table 4).
| Observer | True positives | False positives | True negatives | False negatives |
| A.F. with NIRT | 197 | 76 | 2490 | 194 |
| F.R. with NIRT | 161 | 36 | 2530 | 230 |
| A.F. with RE | 277 | 336 | 2224 | 114 |
| F.R. with RE | 192 | 44 | 2522 | 199 |
| Sensitivity | NIRT | RE | P |
| A.F. data | 0.504 | 0.699 | P<0.001 |
| F.R. data | 0.408 | 0.484 | P=0.029 |
| All data | 0.456 | 0.591 | P<0.001 |
RE specificity to caries detection without clinical evaluation by the same operators was 0.883 and 0.984, respectively. NIRT specificity was 0.973 and 0.987, respectively. The specificity of NIRT was higher than the RE specificity when the analysis was performed by A.F. (p<0.001), but the difference was not significant in the analysis performed by F.R. (p=0.295) (Table 5).
If aggregate data were examined, RE performed significantly better than NIRT in sensitivity analysis (p<0.001) and NIRT performed significantly better than RE in specificity analysis (p<0.001) (Table 4, Table 5).
| Specificity | NIRT | RE | P |
| A.F. data | 0.973 | 0.883 | P<0.001 |
| F.R. data | 0.987 | 0.984 | P=0.295 |
| All data | 0.98 | 0.933 | P<0.001 |
Regarding the consistency between the two observers, NIRT performed significantly better than RE (0.901 by RE analysis, 0.989 by NIRT analysis, P<0.001). Sensitivity, which was calculated separately for E1, E2 and D1/D2 caries, is summarized in Table 6. RE performed better than NIRT in E1 diagnosis, but the difference was not statistically significant (p=0.125). NIRT performed slightly better than RE in E2 diagnosis, but the difference was not statistically significant (p=0.928). In D1/D2 diagnoses, RE performed significantly better than NIRT (p=0.001).
| Sensitivity | NIRT | RE | P |
| E1 | 0.313 | 0.435 | P=0.125 |
| E2 | 0.565 | 0.557 | P=0.928 |
| D1/D2 | 0.516 | 0.808 | P<0.001 |
A high probability of false positives in RE was observed for E1 caries (95% CI for false positives ranged from 0.699 to 0.791, mean value 0.748). NIRT is likely to be able to correct a false positive diagnosis for small carious lesions (E1-E2) performed with RE (95% CI in probability of false positives in E1, corrected with NIRT, ranged from 0.938 to 0.979, mean value 0.964).
DiscussionTop
The validation of the accuracy and effectiveness of a diagnostic tool is a key step before the tool can largely be introduced in clinical use. Sensitivity and specificity of the provided results, along with their reproducibility, are central aspects in studies aimed at validating such tools.
To our knowledge, no study has yet investigated NIRT performance in vivo in such a large number of dental surfaces and with a blind experimental project. We chose to evaluate the method by resorting to a group of patients attending a private practice for a physical dental visit. The number of patients was not large, but because we used single interproximal surfaces as statistical units, we gathered data over 2957 statistical units, which enabled us to obtain evaluations with a high statistical significance.
We chose inclusion criteria that allowed us to include patients on whom NIRT evaluation could be performed at least in a posterior quadrant. We considered 276 patients, 162 of which were excluded. The high number of patients who were excluded proves that, at least in Northern Italy, the dental health condition of most adult patients restricts the use of the tool involved in this study, given the high predominance of dental restorations, such as interproximal restorations and full crowns or edentulous cases, which make transillumination devices useless. The recruited patients had an average age (32.5) much lower than that recorded by the overall patients taken into account (44). This provides evidence that the oldest patients do not match the inclusion criteria. It may therefore be stated that the scope of NIRT in diagnosing caries is more limited compared with RE because it cannot be used to evaluate secondary caries on teeth that have been previously treated.
The sensitivity and specificity assessment of a diagnostic test must be based on a reference diagnosis. Today no definitive diagnostic gold standards have been defined in caries detection [18]. In this study, the reference diagnosis was made, as stated, during the physical visit performed by two well-experienced operators who resorted to visual-tactile, RE and NIRT examinations simultaneously. More objective methods, as temporary tooth separation, have been described for experimental studies in caries detection [19]. However this method has been described for primary molars and it would be difficult to implement on the teeth of adult patients. Above all in a large private practice sample, the fact we not used an absolutely objective method for caries reference diagnosis, is a sure source of bias of this work.
The sensitivity and specificity values that were calculated for RE on the basis of data provided by the two medium-experienced operators are absolutely consistent with previous publications [9], and this, coupled with the fact that the preliminary assessment showed a high agreement, confirms that the observers that we had chosen were fit for the experimental evaluations.
The results show that NIRT had significantly less sensitivity compared with RE, but significantly more specificity. Furthermore, consistency among operators was significantly higher for NIRT, even though it must be noted that the agreement was considerable in both methods. When considering the evaluation over the different caries depths, the two methods show similar sensitivity to E1 and E2 caries, whereas RE proves to be more sensitive to dentin caries. Because it is generally agreed that dentin caries, to which NIRT proves to be significantly less sensitive, must be treated with restorations, they will not be monitored over time in order to evaluate caries progression. Only enamel caries will be medically treated and monitored, as this study seems to demonstrate that in this case, NIRT and RE sensitivity are similar. If these data are confirmed while following-up enamel caries, NIRT could replace RE, in the interest of patients, who would be less exposed to ionizing radiation. This is even more true in high-caries-risk individuals, on whom not all specialists agree to perform a medical approach [20] and for whom a frequent follow-up is therefore mandatory, which, if carried out by resorting to RE, would cause significant exposure to X-rays.
It must be clarified that the experimental observations of this study were made on static images (just one image for each interproximal surface), whereas NIRT provides dynamic images in real time, which should enable more accurate analysis. This depends on the fact that the sensor can be moved around and tilted to examine each interproximal zone from many perspectives and to perform more accurate examinations. There is no doubt that such a point of view is a bias of our evaluation, which might have underestimated the sensitivity of the device.
An interesting factor concerns the high probability of making false positive diagnoses using RE in the case of enamel caries (E1), given that consistency among observers is particularly poor (0.605, 95% CI from 0.525 to 0.681) on this point.
In this regard, we wanted to calculate how likely NIRT was to disclose such false positives, and the probability was proven to be very high (0.964, 95% CI from 0.938 to 0.979). These values suggest that transillumination can be used to confirm the diagnosis of early interproximal enamel caries detected with RE.
Furthermore, we wish to stress that the authors have personally experienced how NIRT, by providing three-dimensional images, can deliver useful operating suggestions, which enable the performance of a targeted cavitation into the dental crown and the ability to reach small caries with precision and good restorative results in a less invasive manner.
A bias of this study is the absence of a clinical validation of caries that would have provided the certainty of the diagnosis. Additional studies are required to obtain this validation.
ConclusionTop
Assuming that NIRT does not match RE because it is not able to provide information in cases of previous restorations performed on the surfaces of the element being examined, the method seems to perform in a comparable, and sometimes even better, manner than RE in the diagnosis of interproximal caries of non-restored teeth. In particular, this diagnostic device could be used to monitor caries restricted to enamel over time, to make diagnoses in patients who should not be exposed to ionizing radiation unless absolutely necessary (e.g., pregnant women and children), or to confirm the diagnosis of non-cavitated caries made by means of RE. The device can also provide information on the three-dimensional location of small caries, making the treatment more conservative.
Conflicts of interest
The authors hereby declare that they have no conflicts of interest.
ReferencesTop
[1]Jefferies SR. Advances in remineralization for early carious lesions: a comprehensive review. Compend Contin Educ Dent. 2014; 35(4):237–243.Pubmed
[2]Cochrane NJ, Cai F, Hug NL, Burrow MF, Reynolds EC. New approaches to enhanced remineralization of tooth enamel. J Dent Res. 2010; 89(11): 1187–1197.Article Pubmed
[3]Frencken JE, Peters MC, Manton DJ, Leal SC, Gordan VV, et al. Minimal intervention dentistry for managing dental caries – a review: report of a FDI task group. Int Dent J. 2012; 62(5): 223–243.Article Pubmed
[4]Yang J, Dutra V. Utility of radiology, laser fluorescence and transillumination. Dent Clin North Am. 2005; 49(4):793–752.Article Pubmed
[5]Wenzel A, Fejerskov O, Kidd E, Joyston-Bechal S, Groeneveld A. Depth of occlusal caries assessed clinically, by conventional film radiographs, and by digitized processed radiographs. Caries Res. 1990; 24(5): 327–333.Pubmed
[6]Syriopoulos K, Sanderink GC, Velders XL, van der Stelt PF. Radiographic detection of approximal caries: a comparison of dental films and digital imaging systems. Dentomaxillofac Radiol. 2000; 29(5): 312–318.Article Pubmed
[7]Astvaldsdottir A, Ahlung K, Holbrook WP, de Verdier B, Tranæus S. Approximal caries detection by DIFOTI: in vitro comparation of diagnostic accuracy/efficacy with film and digital radiography. Int J Dent. 2012.Article Pubmed
[8]Bin-Shuwaish M, Yaman P, Dennison J, Neiva G. The correlation of DIFOTI to clinical and radiographic images in class II carious lesions. J Am Dent Assoc. 2008; 139(10):1374–1381.Article Pubmed
[9]Pretty IA. Caries detection and diagnosis: novel technologies. J Dent. 2006; 34(10):727–739.Article Pubmed
[10]Bader JD, Shugars DA, Bonito AJ. Systematic reviews of selected dental caries diagnostic and management methods. J Dent Educ. 2001; 65(10):960–968.Article Pubmed
[11]Darling CL, Huynh GD, Fried D. Light scattering properties of natural and artificially demineralized dental enamel at 1310 nm. J Biomed Opt. 2006; 11(3):34023.Article Pubmed
[12]Fried D, Glena RE, Featherstone JD, Seka W. Nature of light scattering in dental enamel and dentine at visible and near-infrared wavelengths. Appl Opt. 1995; 34(7):1278–1285.Pubmed
[13]Sochtig F, Hickel R, Kühnisch J. Caries detection and diagnostics with near-infrared light transillumination: clinical experiences. Quint Int. 2014; 45(6):531–538.Article Pubmed
[14]Fellows JL, Gordan VV, Gilbert GH, Rindal DB, Qvist V, et al. Dentist and practice characteristics associated with restorative treatment of enamel caries in permanent teeth: multiple-regression modeling of observational clinical data from the National Dental PBRN. Am J Dent. 2014; 27(2):91–99.Pubmed
[15]Pitts NB. Clinical diagnosis of dental caries: a European perspective. J Dent Educ. 2001; 65(10):972–978.Article Pubmed
[16]Nascimento MM, Bader JD, Qvist V, Litaker MS, Williams OD, et al. Concordance between preoperative and postoperative assessments of primary caries lesion depth: results from the Dental PBRN. Oper Dent. 2010; 35(4):389–396.Article Pubmed
[17]Chu CH, Chau AM, Lo EC. Current and future research in diagnostic criteria and evaluation of caries detection methods. Oral Health Prev Dent. 2013; 11(2): 181–189.Article Pubmed
[18]Baelum V. What is an appropriate caries diagnosis Acta Odontol Scand. 2010; 68(2):65–79.Article Pubmed
[19]Novaes TF, Matos R, Braga MM, Imparato JC, Raggio DP, et al. Performance of a pen-type laser fluorescence device and conventional methods in detecting approximal caries lesions in primary teeth--in vivo study. Caries Res. 2009; 43(1):36–42.Article Pubmed
[20]Kakudate N, Sumida F, Matsumoto Y, Manabe K, Yokoyama Y, et al. Restorative treatment thresholds for proximal caries in dental PBRN. J Dent Res. 2012; 91(12):1202–1208.Article Pubmed
 Copyright
© 2012-2025 NobleResearch Group. All Rights Reserved
Copyright
© 2012-2025 NobleResearch Group. All Rights Reserved