



- Download PDF
- |
- Download Citation
- |
- Email a Colleague
- |
- Share:
-
- Tweet
-
Journal of Radiology and Imaging
Volume 1, Issue 1, July 2016, Pages 9–13
ReviewOpen Access
The forgotten lymph nodes: Review of the superficial head and neck lymphatic system
-
Wessam Bou-Assaly1,*

*Corresponding author: Wessam Bou-Assaly, MD., Department of Radiology, Habib Medical Group, United Arab Emirates. E-mail: wissiba@hotmail.com
Received 9 April 2016 Revised 11 June 2016 Accepted 19 June 2016 Published 27 June 2016
DOI: http://dx.doi.org/10.14312/2399-8172.2016-3
Copyright: © 2016 Bou-Assaly W, et al. Published by NobleResearch Publishers. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
AbstractTop
In patients with head and neck malignancy, knowledge of the lymphatic pathways relevant to tumor location is important for treatment preparation, both in radiation therapy and in surgery. The lymphatics of the head and neck area consist of superficial and deep nodes groups, which are connected by numerous small vessels, giving rise to a complex subcutaneous and deep lymphatic network. The deep cervical lymph nodes, mainly placed along the jugulo carotid vessels, have been intensively reviewed in radiology and classified by well-established levels. The more superficial groups, notably the occipital, parotid, mastoid, facial and superficial cervical lymph nodes groups were not well recognized in the radiology literature, probably because of their less frequent involvement in the more predominant pharyngeal and laryngeal mucosal malignancy, and seem to have been forgotten. We present a review of the anatomy of those lymph nodes groups, including their location, afferent and efferent drainage tracts accompanied by cross-sectional imaging CT examples.
Keywords: lymph nodes; head and neck; lymphatic system
IntroductionTop
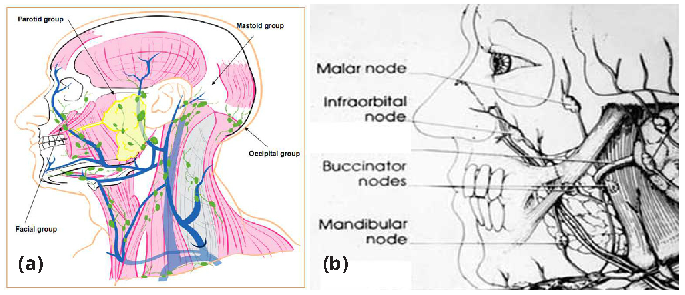
Rouvière classified the lymph nodes of the head and neck into 10 groups. The most superficial ones, namely the occipital, parotid, facial and mastoid groups, situated at the junction of head and neck, form a veritable lymphoid collar that he designated as pericervical lymphoid ring (Figure 1a) [1, 2]. These lymph nodes are intercalated along the course of the lymphatic vessels that drain specific regions along the face, head and neck. Cancer cells carried by blood can end in any organ of the body, but spread through the lymphatic spread is usually stepwise, through successive nodal stops. Knowing the lymphatic pathway becomes thus relevant to any tumor or infection, for treatment preparation and execution [3]. The purpose of this review is to describe the anatomy of the superficial lymph nodes of the head and neck region, their usual location as well as their major afferent and efferent draining pathways.
Facial lymph nodesTop
The facial lymph nodes are the most inconsistently present lymph nodes in the head and neck region. These nodes are found in the subcutaneous planes of the face, deep to the superficial muscles of facial expression (Figure 1b), usually along the course of the facial artery and vein [1, 2]. Rouvière divided the facial nodes into four groups: i. inferior maxillary nodes; ii. buccinator nodes; iii. infraorbital or nasolabial nodes; and iv. malar nodes [1].
Inferior mandibular group
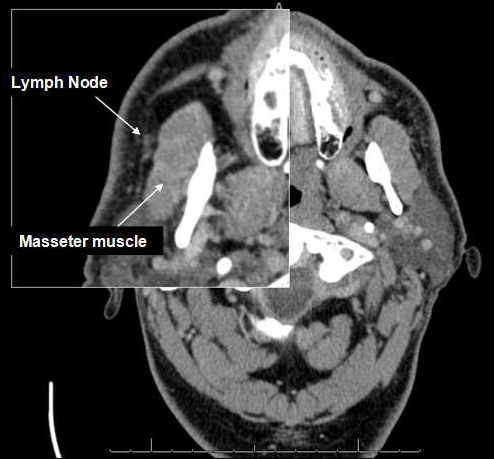
The inferior mandibular group lymph nodes lie along the external surface of the mandible anterior to, or along the external surface of the masseter muscle, or on the mandibular insertion of the buccinator, usually in front of the facial vein (Figure 2). Synonyms for this group include supramaxillary nodes, supramandibular nodes and inframandibular nodes [1, 4].
The mandibular lymph nodes has its afferent drainage from the infraorbital and buccinator lymphatics as well as from the skin and subcutaneous tissues of the cheek, lower lip, and less commonly the gingiva, buccal mucosa, hard and soft palate. The efferent drainage is to the submandibular lymph vessels and nodes [1, 4, 5].
These nodes are also of most interest to the head and neck surgeon, since they could be involved, even though rarely reported, in head and neck cancer [5]. Sheahan et al., reported their involvement in palatine tonsils, retromolar trigon, base of the tongue and floor of the mouth malignancy. A striking findings with mandibular lymph nodes metastasis from head and neck cancer, is their association with a singular poorer outcome, with the survival rate dropping to 14.3 % in patients with positive facial nodes from 62.5 % for patients with negative facial nodes [5].Buccinator group
The buccinator group lymph nodes are found overlying the buccinator muscle and its fascia, or in the fat of the buccinator space (Figure 3). These are divided into two groups according to their relationship to the anterior facial vein. The anterior nodes lie anterior or superficial to the facial vein, whereas the posterior subgroup is placed posterior or deep to it, in the vicinity and below the point of entry of the Stenson’s duct in the buccinators [1, 4].

The afferent drainage of the buccinator lymph nodes is from the skin and subcutaneous tissues of the lower eyelid, nose, cheek, and rarely the temporal region. The efferent drainage is by the mandibular lymphatics to the submandibular lymph vessels and nodes [1, 4].
Infraorbital or nasolabial group
The infraorbital or nasolabial group lymph nodes are rarely present and when they are, usually represented by one small node along the facial artery or anterior facial vein, in the nasolabial fold or in the canine fossa near the fold at the level between the nares and medial canthus of the eye (Figure 4) [1]. Lymphoma has propensity for involving this region and in most cases the lymph node is adherent to the infraorbital neurovascular bundle [4].

The afferent drainage of the infraorbital or nasolabial group of lymph nodes is from the skin and subcutaneous tissues of the medial part of the lids, medial canthus of the eye, nose and nasolabial folds. The efferent drainage is to the buccinator and mandibular lymphatics [1, 4].
Malar group
The malar groups of lymph nodes are found superficial to the malar eminence, intercalated along the vertical lymphatic channels coursing from the parotid, over the zygomatic arch, to the temporal region. Therefore these nodes can be found from the malar eminence to the end of the zygomatic process [1, 4].
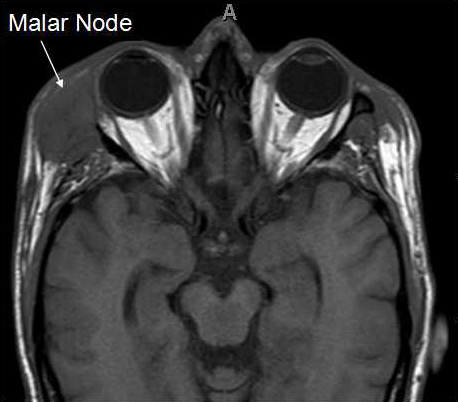
The afferent drainage of the malar lymph nodes is from the skin and subcutaneous tissues of the lids, lateral canthus region, and temporal region, with the efferent drainage to the parotid nodes [1, 4].
Overall, the facial lymph nodes drain the skin and subcutaneous tissues of the face, eyelids, region of medial and lateral canthi, conjunctiva, skin and mucous membrane of the nose and cheek and drain into the submandibular group, with the exception of the malar nodes which drain into the parotid lymphatics. The mandibular lymph nodes have also some deeper afferent drainage from the gingiva and buccal mucosa.
Occipital lymph nodesTop
The occipital lymph nodes, 1 to 10 in number, are divided into 3 groups; suprafascial, subfascial and deep occipital nodes [1, 3].
Suprafascial group
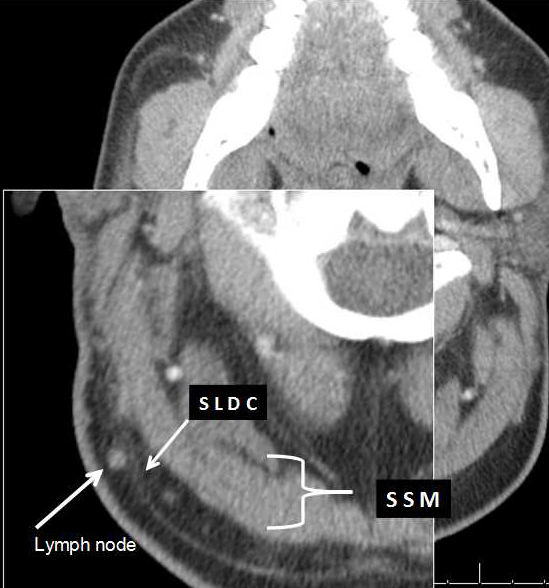
The suprafascial or superficial group, are intimately applied to the superficial layer of the deep cervical fascia or to the epicranial aponeurosis (Figure 6). They are usually found along the third part of the occipital artery and great occipital nerve. This explains why superficial occipital lymphadenitis may lead to neuralgia or neuritis of this nerve [1, 2]. They are usually located at posterosuperior angle of the sternocleidomastoid (SCM) and between the insertion of the SCM and trapezius.
Those lymph nodes are the most common occipital nodes and count for around 63 % of the identified nodes [6].
Subfascial group
The subfascial group lies near the superior nuchal line of the occipital bone, beneath the superficial layer of the deep cervical fascia (Figure 7) [1, 2].
Deep occipital groups
The submuscular or subsplenius or deep occipital groups are more constant in location. They lie beneath the superior insertion of splenius capitis, above obliquus capitis superior and medial to the longissimus capitis [1, 2] (Figure 8).
Afferent and efferent drainage
The occipital lymph nodes drain the occipital part of scalp (posterior part of the hairy scalp), skin of the upper part of the nape of neck and also, by means of subfascial and subsplenius, a portion of the deep layers of the neck which borders on the occipital region. The efferent vessels run from occipital nodes to the deep lateral nodes of the neck, mainly nodes of spinal accessory chains. Some vessels run obliquely from superficial or subfascial occipital nodes to the nodes of spinal accessory chain, placed at different levels, under the SCM and near its posterior border, or in the supraclavicular triangle [1-3].
Parotid lymph nodesTop
Parotid lymph nodes are divided into three groups determined by the embryological development of the parotid gland. i. Superficial extrafascial; ii. Subfascial extraglandular; and iii. Deep intraglandular nodes.
Superficial extrafascial group
The superficial extrafascial group nodes are located superficial to the superficial layer of the deep cervical fascia. They are usually preauricular placed close to the tragus but can be located along the notch between the tragus and antitragus (Figure 9) [1, 2].

The superficial extrafascial as well as the subfascial preauricular nodes discussed below, receive nearly all lymph vessels from frontal part of cranial vault, root of the nose, upper and lower lids, auricle and external auditory. Quite often, lymphatic network of the Eustachian tube partly drains by a superficial parotid node or subfascial node, through the intermediacy of lymphatic network of tympanic membrane and collecting vessels along EAC [1].
The subfascial extraglandular group nodes are immediately below the fascia, contained in the parotid sheath but not included in the parotid glandular tissue.
Rouviere divided them into subfascial preauricular and infra-auricular nodes. The first group, preauricular, is located between the fascia and the parotid gland parenchyma, near the tragus and in front of the auricle. This group has grossly similar drainage pattern as the superficial extrafascial nodes.
The more inferior infra-auricular group is usually located in the region of external jugular vein, where it exits the parotid gland and located between inferior extremity of the parotid and anterior border of the sternocleidomastoid muscle (Figure 10) [1, 2].
This group receives the lymphatic from the posterior part of cheek, parotid gland, the nose, upper lid, buccal mucous membrane, as well as the efferent lymph vessels from external ear, from the mastoid space nodes, and from parotid groups [1, 2].
Deep intraglandular group
The deep intraglandular group nodes are located in the cellular tissue of the parotid gland, usually between the superficial and deep lobes of the parotid (Figure 11) [1, 2]. Pathological studies have shown that most of them lie lateral to the retromandibular vein and not the facial nerve, thus any dissection that follows the nerve may leave residual disease [7].
The intraglandular nodes receive some lymph vessels originating from the skin of the frontal and temporal regions, lateral parts of the lids, from the lacrymal gland, external auditory canal, tympanic membrane and eustachian tube, and lastly, a part of the efferent vessels from the superficial preauricular nodes [1, 2].
Overall the parotid lymph nodes drain the frontal and temporal cranial vault, the nose, upper and lower lids, auricle and external auditory, tympanic membrane and part of the eustachian tube, superficial preauricular nodes, posterior part of cheek, parotid gland, external ear, mastoid space nodes and lacrymal glands.
The parotid gland is also involved in metastases from oropharyngeal and nasopharyngeal malignancies that may affect both superficial and deep intraglandular lymph nodes [7]. Squamous cell carcinomas are reported to metastasize to the parotid lymph nodes with the incidence higher with patients who have positive surgical margins, advanced tumor stages and those who didn’t receive adjuvant irradiation [7].
Rouviere described three principle efferent pathways connecting and draining the parotid lymph nodes [1]. The posterior or retroglandular path commences in the pretragus nodes and runs along posterior borders of the parotid gland and terminates in a node of the internal jugular chain, directly or by intermediary of one of the inferior parotid subfascial nodes.
The venous path involve an efferent vessel originating from the superficial or the subfascial preauricular lymph nodes, and ends in an intraglandular lymph node, near branches of the external jugular vein. The path descends along this vein and terminates in a node of the internal jugular chain.
The arterial path takes origin in a preauricular node, particularly in a pretragus node, joins branches of the external carotid artery and then descends along this artery and terminates in a node of the internal jugular chain.
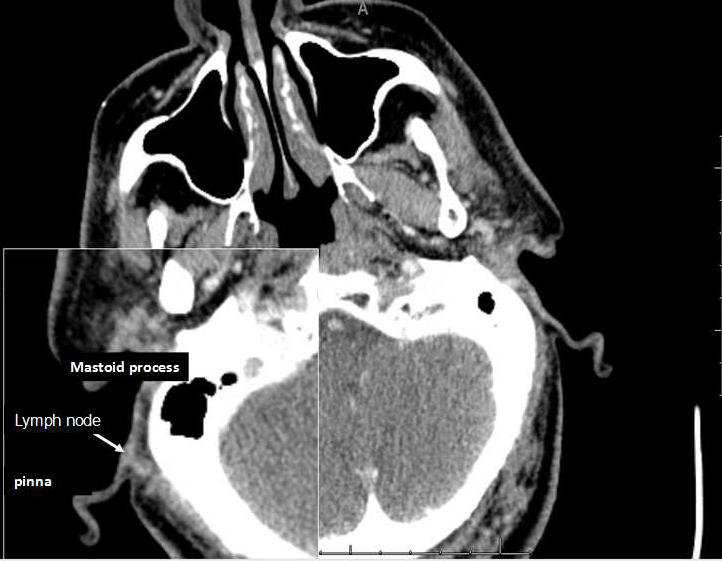
Mastoid lymph nodesTop
Mastoid lymph nodes (Figure 12) are located in retroauricular area, in the mastoid region. They are more numerous in children than adults and they lie superficial to the attachment of the SCM [1, 2].
Afferent and efferent draining
The mastoid lymph nodes usually drain lymph vessel issuing from the parietal and temporal region of the scalp, posterior surface of the auricular and posterior wall of the external acoustic meatus [1, 2].
Some of those nodes have their efferent vessels empty into the inferior parotid subfascial nodes; some traverse the SCM to drain in the superior deep lateral cervical lymph nodes.
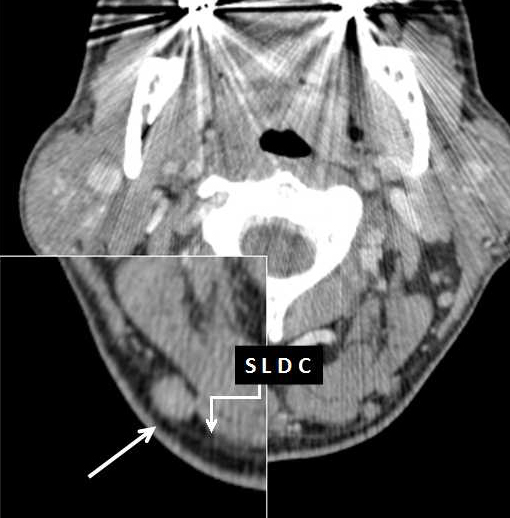
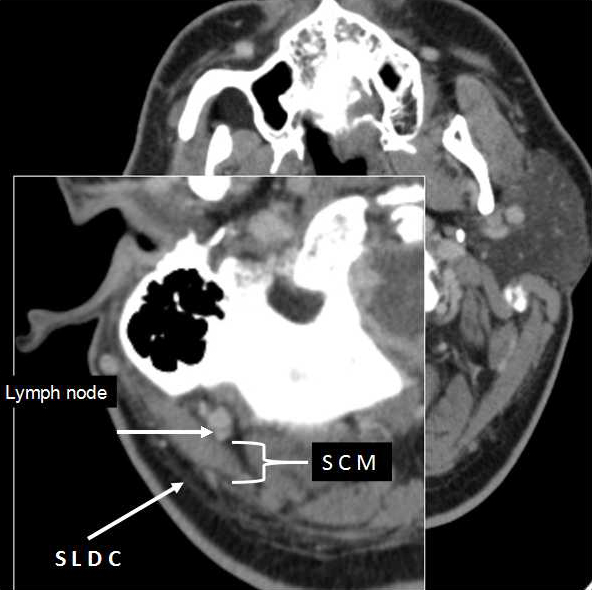
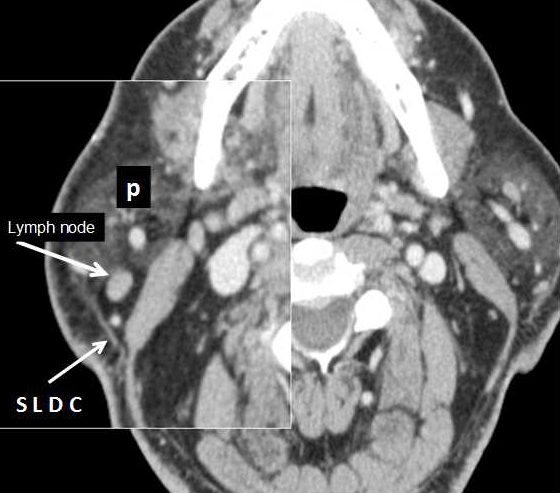
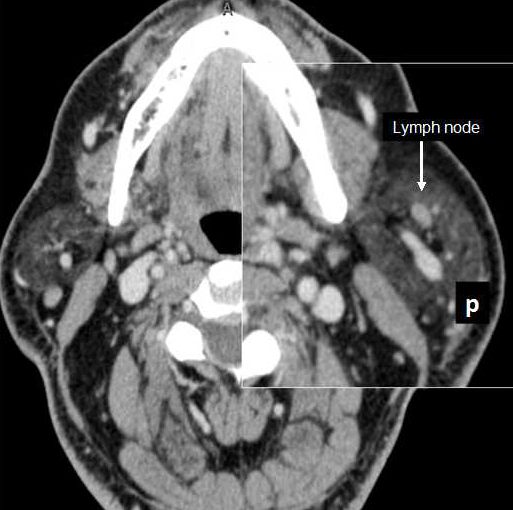
Superficial cervical lymph nodesTop
These nodes lie in close relationship with the external jugular vein as it emerges from the parotid gland, and, therefore, superficial to the sternocleidomastoid muscles. They are divided as anterior, spread along the anterior jugular vein and posterior found along the external jugular vein [1, 8].
Their afferents drain the lower parts of the auricular and parotid region, while their efferents pass around the anterior margin of the sternocleidomastoid muscle to join the superior deep cervical glands [8].
ConclusionTop
In this presentation, we reviewed the superficial groups of the head and neck lymph nodes, notably the occipital, parotid, mastoid and facial lymph nodes, including their anatomic locations and major afferent and efferent drainage tracts. Those node groups seem to have been forgotten by the radiology literature, which has more intensively reviewed the deep lymphatic network.
Conflicts of interest
Author declares no conflicts of interest.
ReferencesTop
[1]Rouviere H, Tobias MJ. Anatomy of the human lymphatic system. Ann Arbor, Edwards Brothers. 1938.
[2]Lengelé B, Hamoir M, Scalliet P, Grégoire V. Anatomical bases for the radiological delineation of lymph node areas. Major collecting trunks, head and neck. Radiother Oncol. 2007; 85(1):146–155.Article Pubmed
[3]Pan WR, Suami H, Taylor GI. Lymphatic drainage of the superficial tissues of the head and neck: anatomical study and clinical implications. Plast Reconstr Surg. 2008; 121(5):1614–1624.Article Pubmed
[4]Tart RP, Mukherji SK, Avino AJ, Stringer SP, Mancuso AA. Facial lymph nodes: normal and abnormal CT appearance. Radiology. 1993; 188(3):695–700.Article Pubmed
[5]Sheahan P, Colreavy M, Toner M, Timon CV. Facial node involvement in head and neck cancer. Head Neck. 2004; 26(6):531–536.Article Pubmed
[6]Veenstra HJ, Klop WM, Lohuis PJ, Nieweg OE, van Velthuysen ML, et al. Cadaver study on the location of suboccipital lymph nodes: Guidance for Suboccipital node dissection. Head Neck 2014; 36(5):682–686.Article Pubmed
[7]Wang S, Lou J, Zhang S, Guo L, Wang K, et al. Metastasis of nasopharyngeal carcinoma to parotid lymph nodes: a retrospective study. World J Surg Oncol. 2015; 13:1.Article Pubmed
[8]Henry Gray. Anatomy of the human body. 20th ed., rev. and re-edited by Warren H. Lewis. The lymphatic system: The lymphatics of the head, face, and neck, pp 1396.
 Copyright
© 2012-2019 NobleResearch Group. All Rights Reserved
Copyright
© 2012-2019 NobleResearch Group. All Rights Reserved