



- Download PDF
- |
- Download Citation
- |
- Email a Colleague
- |
- Share:
-
- Tweet
-
Journal of Radiology and Imaging
Volume 2, Issue 2, February 2017, Pages 11–13
Case reportOpen Access
The hydrocele of canal of Nuck: Case report and review of the literature
-
Bou-Assaly W1,*

*Corresponding author: Wessam Bou-Assaly, MD, Department of Radiology, Habib Medical Group, DHCC, Dubai, United Arab Emirates. Tel.: +971-554877488; E-mail: wissiba@hotmail.com
Received 09 Decmber 2016 Revised 18 January 2017 Accepted 25 January 2017 Published 29 January 2017
DOI: http://dx.doi.org/10.14312/10.14312/2399-8172.2017-3
Copyright: © 2017 Bou-Assaly W, et al. Published by NobleResearch Publishers. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
AbstractTop
The hydrocele of the canal of Nuck is a rare condition that results from the failure of obliteration of the distal portion of evaginated parietal peritoneum within the inguinal canal which forms a sac containing fluid. It usually presents with painless inguinal swelling that may lead to investigation by imaging, mainly ultrasound, CT or MRI. We present a case of a 30-year-old female who presented for a 2-3 cm right inguinal canal hydrocele of the canal of Nuck, followed by review of the literature.
Keywords: hydrocele of canal; Nuck; peritoneum
IntroductionTop
The canal of Nuck is homologous to processus vaginalis in men. It is a small pouch of patent peritoneal fold extending along the round ligament into the inguinal canal, through the inguinal ring. It undergoes complete obliteration during the first year of life [1]. Incomplete obliteration results in fluid trapped in the peritoneal remnant, forming a hydrocele of the canal of Nuck and failure of obliteration may result in inguinal hernia [1].
Case reportTop
A 30-year-old female patient was referred to our surgical department by her gynecologist for a suspected right inguinal hernia. She had a moderately painful swelling in her right groin, palpable up to 3 cm, which she had noticed a week ago. She had no fever, or any gastrointestinal symptoms.
Physical examination revealed a localized fluctuant mass in the region of her right inguinal canal that does not increase on the Valsalva maneuver and cannot be reduced by manual pressure. The mass was transilluminant, with no thrill or bruit with and normal overlying skin with no associated inflammation. There were no symptoms of bowel obstruction or other abdominal disease.
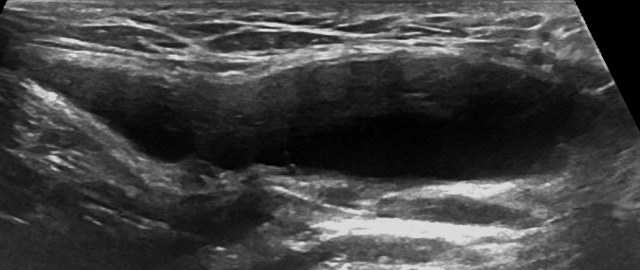
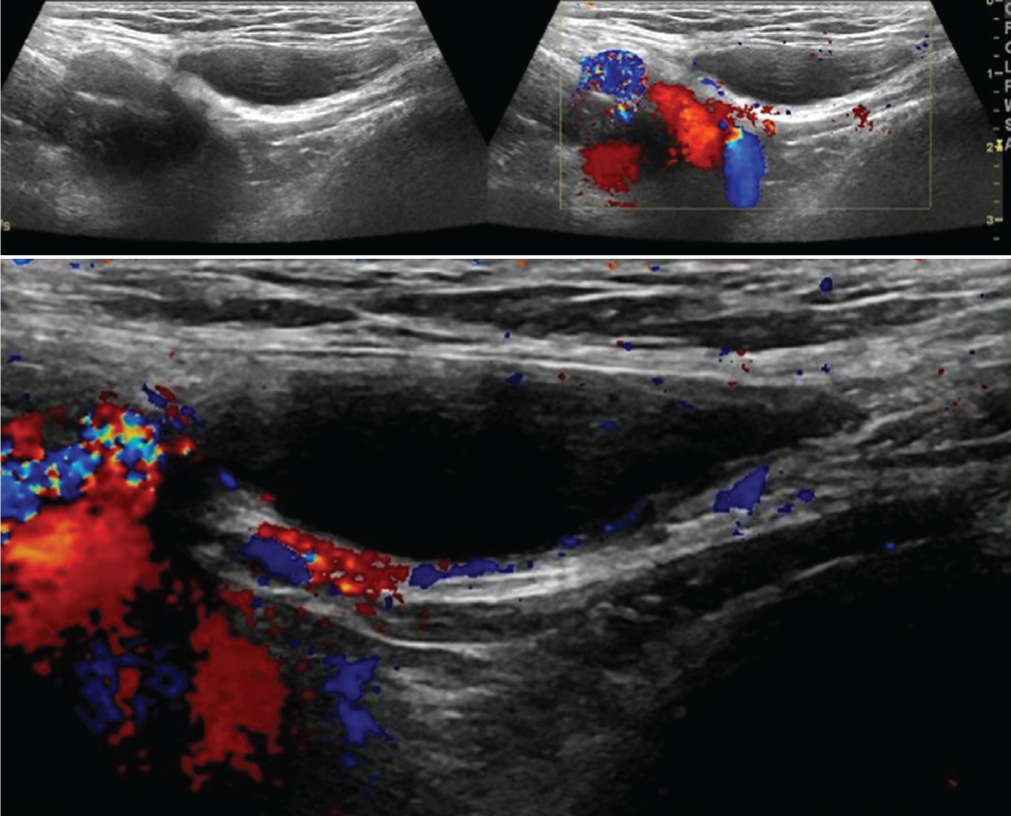
Pelvic ultrasound showed a 3.5 × 2.6 cm oval shaped completely cystic lesion, with fine echogenic margins, located within the right inguinal region, without internal soft tissue component or vascular structure, without obvious communication with the abdominal cavity (Figures 1 and 2).
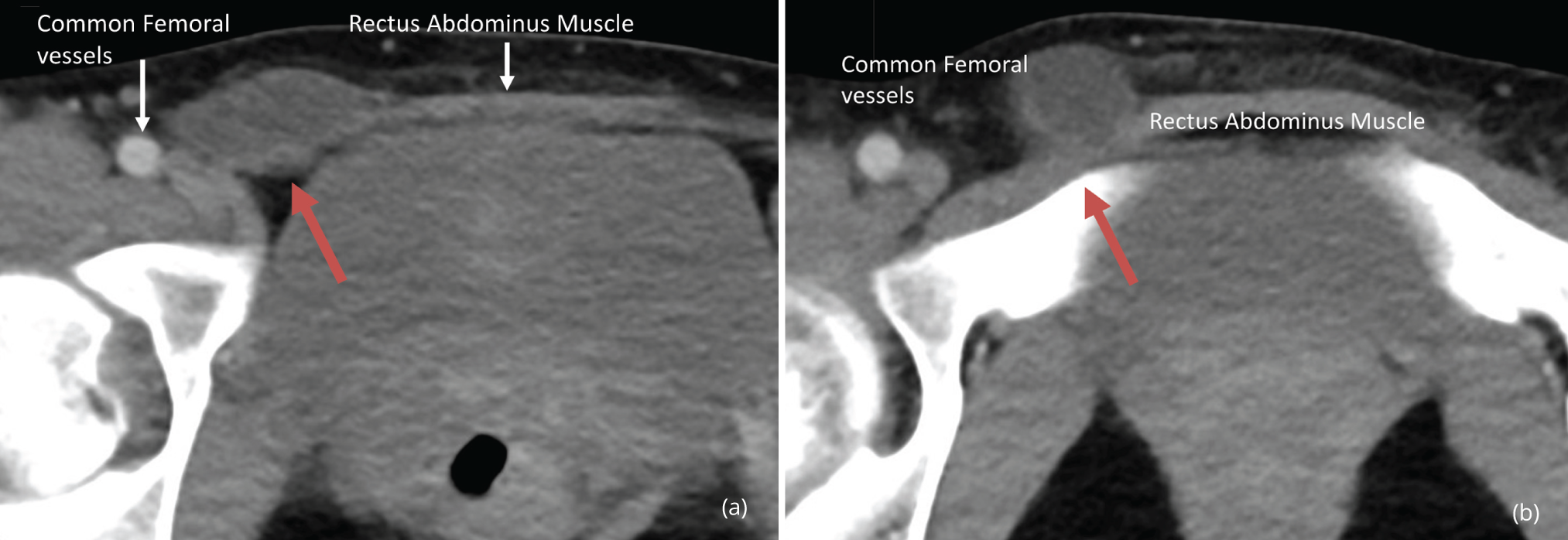
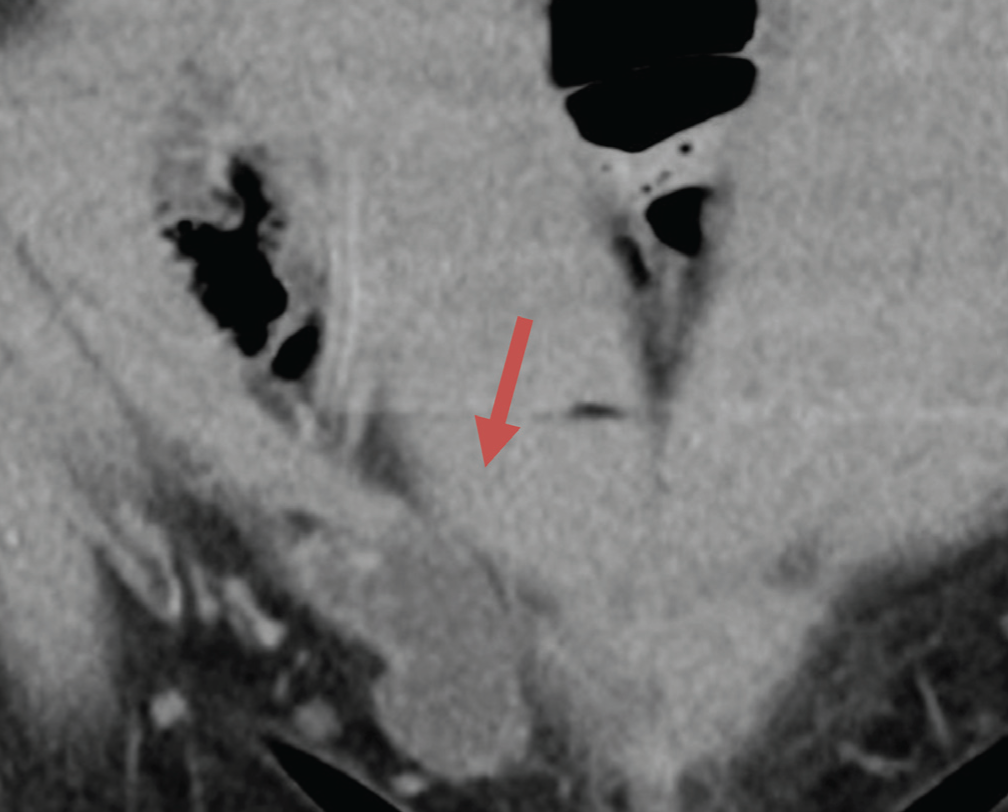
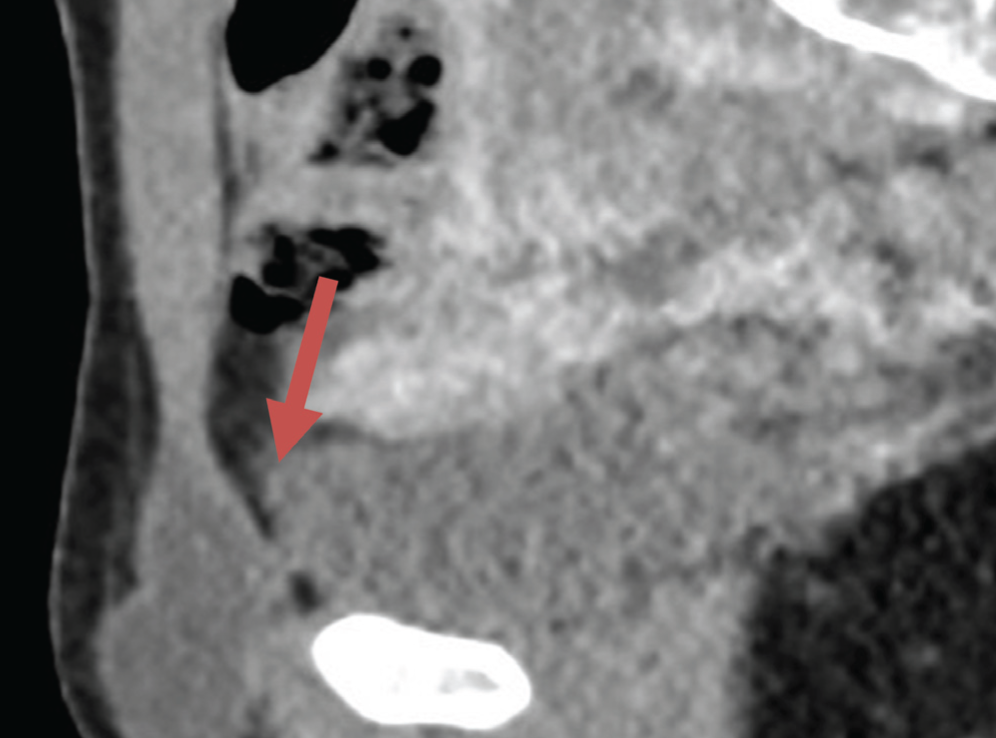
Given the lack of obvious communication with the abdominal cavity, the pain associated with the lesion and the uncertainty about possible association with an inguinal hernia, a contrast enhanced abdomen and pelvic CT was obtained that demonstrates a similar 3.5 cm tubular-shaped fluid density lesion at the right inguinal canal, without obvious communication with the peritoneal cavity, extending inferiorly into the suprapubic area (Figures 3, 4 and 5). No soft tissue or vascular components were identified in the mass lesion. The lesion was removed surgically and histopathology revealed the diagnosis of hydrocele of canal of Nuck, with fibrous tissue and flattened mesothelial cells lining the inner surface of a completely cystic lesion, with clear amber fluid, with no internal cells or microorganism.
DiscussionTop
The processes vaginalis within the inguinal canal in women is called the canal of Nuck. This was first described by the Dutch anatomist Anton Nuck in 1691 [1]. The inguinal canal is traversed by the spermatic cord in men and the round ligament of uterus in women. The round ligament is attached to the uterine cornu at one end and to the ipsilateral labia majora at the other and accompanies a pouch of parietal peritoneum in the inguinal canal, known as ‘canal of Nuck’, analogous to the processus vaginalis [2, 3].
The canal of Nuck usually gets obliterated by birth or during early infancy, gradually in a downward direction, but if this communication remains patent, it may lead to development of an indirect inguinal hernia or hydrocele [1, 2, 4, 5]. Some authors assume that obliteration of the processus vaginalis occurs after the seventh month of gestation, thus accounting for the higher incidence of inguinal hernias in the premature infant [6].
The hydrocele of the canal of Nuck is a very rare condition and results from the incomplete failure of obliteration of the distal portion of the canal [1, 2]. An imbalance of fluid secretion and absorption by the secretory membrane lining the processus vaginalis leads to the development of a fluid containing sac [3]. This process is idiopathic in most cases but also can be caused by inflammation, trauma or impairment of lymphatic drainage [5]. The hydrocele of the canal of Nuck generally manifests as a painless swelling in the inguinal area and labium in adolescent age groups. Occasionally it may present with dull aching pain.
The hydrocele of canal of Nuck is classified into three types [2]: (i) The most common type is the encysted type where there is no communication of the hydrocele with the peritoneal cavity and the cyst may be found anywhere along the course of the round ligament from the deep ring to the labia majora. (ii) The second type is similar to congenital hydrocele seen in male where there is a persistent communication between hydrocele and the peritoneal cavity. (iii) In third variety there is a constriction at the deep ring like an hour-glass, so that the proximal part of the sac is retroperitoneal and the distal portion of the sac is in the inguinal canal and clinically simulates an inguinal hernia.
The differential diagnosis of inguinal masses in a young female patient include Bartholin’s cyst, lymphadenopathy, indirect inguinal hernia, post-traumatic hematoma and malignant and benign tumors including lipoma, vascular aneurysm, sarcoma and rarely cystic lymphangioma, leiomyoma and epidermal cyst [1, 2, 5]. Hydrocele of canal of Nuck may be misdiagnosed as inguinal hernia because of its rarity, lack of clinician’s knowledge regarding this entity and paucity of the relevant literature in the surgical textbooks. Furthermore at least one third of the cases are associated with inguinal hernia and most of the cases reported in the literature were diagnosed at surgery performed for suspicious inguinal hernia [7, 8].
Complications of the hydrocele of the canal of Nuck are infection, hemorrhage, or a large cyst with retroperitoneal extension [1]. Multiloculated hydroceles are reported in female as well as in male patients, so internal septations are obviously not uncommon [3]. Rarely, herniation of the urinary bladder, ovary, and fallopian tubes into the canal of Nuck has been reported [4].
Ultrasound is usually the first and preferred investigation due to its availability and the superficial location of the lesion [1]. The lesion is typically seen as a well-defined hypo-echoic or anechoic, sausage- or comma-shaped mass lying superficially and medial to the pubic bone in the inguinal canal with enhanced posterior through translucency [1]. CT and Magnetic resonance imaging (MRI) are not usually necessary if clinical examination and ultrasound are conclusive. They are usually in inconclusive cases or to rule out a possible associated inguinal hernia. CT will demonstrate a non-enhancing cystic lesion, with no communication with the abdominal cavity. The MRI findings include a well-defined, thin-walled, sausage shaped cystic lesion, which is hypointense on T1 and hyperintense on T2-weighted images without internal enhancement [1, 2].
Surgery is necessary for final diagnosis and treatment and considering common association with indirect inguinal hernia [2]. Surgical dissection must be done up to the deep inguinal ring along with high ligation of the neck of the peritoneal pouch. Laparoscopy was also used for diagnosis as well as treatment of this entity [7].
Sonographically guided aspiration can be used to temporarily alleviate patient discomfort in this absolutely benign condition [3]. The histologic composition of a cyst of the canal of Nuck reflects its peritoneal origin: A variously thick fibrous outer wall containing blood vessels and occasionally smooth muscle fibers, lined on the inside with a single layer of mesothelial cells [3].
ConclusionTop
Hydrocele of the canal of Nuck, even though a rare entity should be considered as a differential diagnosis in a girl or young female adult presenting with swelling in the inguinal region. Diagnosis may not be possible only on physical examination and further evaluation with ultrasound, CT or MRI scan imaging will be helpful to reach a definitive diagnosis and also help ruling out an associated inguinal hernia. The treatment of choice for hydrocele of canal of Nuck is complete surgical excision, although sonographic guided aspiration can be used to temporally alleviate the patient’s discomfort.
Conflicts of interest
The author declares no conflicts of interest.
ReferencesTop
[1]Manjunatha YC, Beeregowda YC, Bhaskaran A. Hydrocele of the canal of Nuck: Imaging findings. Acta Radiol Short Rep. 2012; 1(3): arsr.2012.110016.Pubmed
[2]Sarkar S, Panja S, Kumar S. Hydrocele of the canal of Nuck (female hydrocele): A rare differential for Inguino-Labial swelling. J Clin Diagn Res. 2016; 10(2):PD21–22.Pubmed
[3]Stickel W, Manner M. Female hydrocele (cyst of the canal of nuck): Sonographic appearance of a rare and little-known disorder. J Ultrasound Med. 2004; 23(3):429–432.Pubmed
[4]Tubbs RS, Loukas M, Shoja MM, Salter EG, Oakes WJ. Indirect inguinal hernia of the urinary bladder through a persistent canal of Nuck: Case report. Hernia. 2007; 11(3):287–288.Article Pubmed
[5]Poghosyan T, Panzegrau B, Ackerman S. Radiological case: Hydrocele of canal of nuck. Applied Radiology. 2014.Article
[6]Choi YM, Lee GM, Yi JB, Yoon KL, Shim KS, et al. Two cases of female hydrocele of the canal of Nuck. Korean J Pediatr. 2012; 55(4):143–146.Article Pubmed
[7]Matsumoto T, Hara T, Hirashita T, Kubo N, Hiroshige S, et al. Laparoscopic diagnosis and treatment of a hydrocele of the canal of Nuck extending in the retroperitoneal space: A case report. Int J Surg Case Rep. 2014; 5(11):861–864.Article Pubmed
[8]Ushakant RS, Ayyar P. Hydrocele of canal of Nuck: A case report. Int Surg J. 2015; 2(3):396–397.Article
 Copyright
© 2012-2025 NobleResearch Group. All Rights Reserved
Copyright
© 2012-2025 NobleResearch Group. All Rights Reserved