



- Download PDF
- |
- Download Citation
- |
- Email a Colleague
- |
- Share:
-
- Tweet
-
Journal of Clinical and Interventional Cardiology
Volume 4, Issue 1, November 2020, Pages 1–3
Case reportOpen Access
Healthy farmer presenting with chest pain and bradycardia during peak COVID season
-
Sharleen Sheau Yee Siu1,*
 , Andrew Norwood1 and
Madhusudhan Chittari Varma1
, Andrew Norwood1 and
Madhusudhan Chittari Varma1
*Corresponding author: Sharleen Sheau Yee Siu, Cardiology Department, Cumberland Infirmary, Newtown Road, Carlisle, CA2 7HY, UK. Tel.: +44 7706924228; E-mail: sharleen.siu@ncuh.nhs.uk
Received 28 August 2020 Revised 1 October 2020 Accepted 8 October 2020 Published 19 October 2020
DOI: http://dx.doi.org/10.14312/2399-8202.2020-1
Copyright: © 2020 Siu SSY, et al. Published by NobleResearch Publishers. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
AbstractTop
This was a patient who got admitted with three related cardiological presentations during the same admission. Initially he presented with an Inferior ST-elevation myocardial infarction (STEMI) and bradycardia. Following primary percutaneous coronary intervention (PPCI) to the right coronary artery (RCA), he was found to be in complete heart block and new onset atrial fibrillation was noted. This case proved to be interesting and challenging at the same time in view of constantly evolving factors during the peak coronavirus disease (COVID-19) pandemic. There was a great deal of uncertainty over the course of patient's illness not only due to cardiological issues, particularly arrhythmias relating to COVID, but also due to high levels of staff illness, rapidly evolving clinical guidance and emergence of data introducing new variables to consider. The clinical team not only dealt with his initial presenting symptom (chest pain- PPCI) promptly and effectively, but also carefully evaluated his subsequent new unexpected symptoms (bradycardia- pacemaker insertion) and new onset angina (further PCI to LAD) with equal vigour and seriousness, resulting in excellent final results for all of his three conditions with complete and total resolution of all symptoms. We therefore managed to discharge him successfully in spite of unusual challenges noted due to the pandemic situation. We managed to observe highest level protective measures, preventing him from acquiring COVID whilst surrounded by COVID positive and suspected patients and staff.
Keywords: acute myocardial infarction; bradycardia; coronary angiogram; percutaneous coronary intervention; pacemaker; coronavirus disease; COVID-19
Case presentationTop
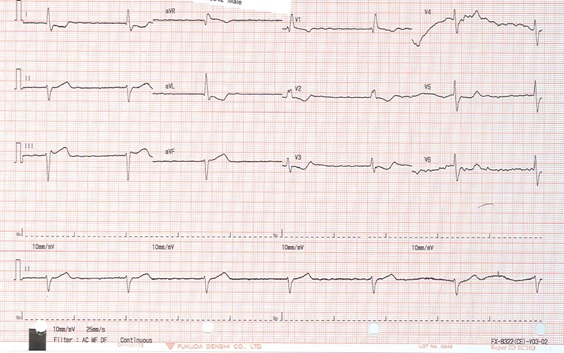
A 82-year-old man presented to hospital with central chest pain occurring at rest. The pain radiated to the left arm with associated sweating and dizziness. His past medical history included polymyalgia rheumatica and gastro-oesophageal reflux disease. On arrival, his electrocardiogram (ECG) demonstrated ST elevation in leads III with mild ST changes in lead II and aVF, ST depression in I, aVL and T wave inversion in V1 to V3 and heart rate of 38 beats per minute (bpm), with no discernible P wave (Figure 1). He was noted to be sinus bradycardic at 34 bpm. Blood pressure was 154/69 mmHg, respiratory rate was 18 bpm and his blood oxygen saturations were 98% on room air.
Troponin T was measured at 176 ng/L, increasing to 1122 ng/L. Other blood tests were unremarkable. The patient denied having any fever or cough and tested negative for COVID-19.
Emergency percutaneous coronary intervention (PCI) was performed within 120 minutes of symptom onset. Atropine was administered during the procedure for his bradycardia. The angiogram revealed blocked distal left posterior descending artery (PDA) of right coronary artery (RCA), severe mid vessel focal calcific lesion of the left anterior descending (LAD) artery and a moderate proximal obtuse marginal (OM1) artery disease. Primary PCI (PPCI) was performed on the distal PDA of the RCA (culprit vessel and lesion) (balloon angioplasty) with successful result in opening of the vessel.
Following the emergency PCI for Inferior STEMI, the patient was monitored in the Coronary Care Unit, Cardiology ward. Echocardiogram demonstrated preserved left ventricular systolic function with an ejection fraction of 50-55%. A routine ECG was undertaken following the procedure which revealed a complete heart block with heart rate of 33 bpm and in atrial fibrillation (AF) (Figure 2). As he now remained symptomatic with profound bradycardia despite waiting for 48 hours post-PCI, a dual-chamber permanent pacemaker was inserted successfully to address his symptoms. A chest x-ray performed following pacemaker insertion confirmed appropriate lead positioning and no related complications. The pacemaker check for pacing parameters was satisfactory and set to VVI as the patient remained in AF.

Following pacemaker insertion and once the heart rate improved from 30 bpm to 60 bpm or higher, the patient now reported typical angina symptoms at rest. He recognised these symptoms (noted only on uphill walking) as stable long standing exertional angina - but now noted at rest. His symptoms continued in spite of starting beta blockers with some effect. Therefore, the LAD lesion also needed to be stented during this admission to relieve his new symptoms (Figure 3).

In view of the newly diagnosed AF, the patient was started on lifelong Apixaban, along with Aspirin for one month and Clopidogrel for twelve months. He was then discharged after successful treatment of his STEMI, complete heart block and AF.
DiscussionTop
This was an interesting case for several reasons. Firstly, we noted more than one cardiac illness which occurred consecutively once each issue was addressed. There was a speculation that COVID-19 exposure/illness could have some bearing on his presentation. It was observed that 9.5% of dying patients with COVID-19 in Italy had developed acute myocardial injury and complications, namely acute coronary syndrome (ACS), arrhythmias, cardiac arrest, heart failure and myocarditis [1].
During this admission, we were in the midst of the COVID-19 pandemic and the United Kingdom (UK) was in lockdown. This also impacted on NHS staff and carers. Our staffing levels were very low. At the same time, there were empty beds in the hospital including our cardiology unit in preparation for a sudden influx of unwell patients.
His baseline 12 lead ECG on admission revealed subtle ST elevation in inferior leads suggesting an Inferior STEMI. Following the angioplasty, the ECG revealed bradycardia of 33 bpm with a regular ventricular rhythm, wide QRS complexes and absent P wave. This indicated AF with a complete heart block. It was unclear whether the MI contributed to the new onset of AF or if the patient had new onset of paroxysmal AF. A recent case report had demonstrated that 7.2% of COVID patients developed acute cardiac injury, 8.7% had shock and 16.7% developed arrhythmias [2]. A dual-chamber pacemaker was fitted for the management of the complete heart block and bradycardia.
At the time of this patient's admission, constant change in guidance for management of cardiac conditions were being debated, released and updated rapidly in view of COVID-19 [3-6]. The NHS also faced constant and daily challenges with sourcing personal protective equipment (PPE) in order to protect staff and patients. A recent article had highlighted the importance of PPE usage. It also suggested that every patient presenting with STEMI requiring PPCI must be treated as suspected COVID-19 until proven otherwise. Primary PCI remained the gold standard management for STEMI’s. Fibrinolysis is considered the next best option [7].
Staff shortages were a major problem. Many of our staff were ill or in isolation after testing positive for COVID-19. As a result, the cardiac catheterisation laboratory was operating with far fewer staff than usual, resulting in working and operating conditions stretched to their limits. Despite these challenges, this patient had a successful outcome with multiple PCI procedures performed and a permanent pacemaker implantation- all in the same admission due to his specific clinical needs.
Finally, our patient was amongst the age group most vulnerable in contracting coronavirus. Those who are over the age of 70, have underlying health conditions or are pregnant are considered higher risk of becoming severely ill from coronavirus [5]. Our coronary care unit (CCU) ward was occupied with patients who were suspected or positive for coronavirus during his stay at our hospital. Despite being surrounded by infectious patients, being in a vulnerable demographic group and staff shortages, our patient remained COVID negative and underwent major procedures, recovered well and is currently healthy and happy.
ConclusionTop
Although the UK and indeed the whole world was going through a pandemic situation from the novel coronavirus with several case reports citing acute myocardial injury and arrhythmia in COVID patients, it was important that we did not assume most cases were related to COVID. It was essential that we treated every clinical problem on its merits appropriately. One needs to be cognisant about the possibility of unmasking further issues once a problem is fixed- as was the case with the pacemaker insertion, it “unmasked” further issue of rate-related angina. This was noted when new angina symptoms developed subsequent to pacemaker insertion (and therefore baseline heart rate improvement to at least 60 bpm) which addressed long standing bradycardia. Since bradycardia was addressed by speeding up the ventricular rate, the background severe disease in the LAD became more relevant in view of reduced diastolic phase and therefore onset of angina symptoms. The onset of arrhythmia post myocardial infarction is not always straightforward. This case highlighted the importance of monitoring patients after acute MI. We were able to adapt and treat according to the patient's symptoms which resulted in the insertion of a pacemaker and a further PCI to his non-culprit lesion and vessel with successful outcome (no further angina). Despite his risk factors including age and major staff shortages, our patient was able to undergo two PCI procedures and a permanent pacemaker implantation within days of admission without contracting coronavirus. This demonstrated excellent work ethic and managing patients using principles of best practice that NHS workers tirelessly adhere to on the frontline to tackle illnesses including the current coronavirus pandemic in supporting their patients. By adhering to proper social distancing guidelines and using scarce and often inadequate PPE kit wisely and appropriately, we managed to demonstrate that best patient care can still be provided even during unprecedented and challenging times.
Conflicts of interest
Authors declare no conflicts of interest.
ReferencesTop
[1]Members of the SARS-CoV-2 Surveillance Group. Characteristics of SARS-CoV-2 patients dying in Italy. Report based on available data on April 13th, 2020. Rome, Italy: Instituto Superiore Di Sanita, 2020. Accessed on 13 May 2020 from: www.epicentro.iss.it/en/coronavirus/bollettino/Report-COVID-2019_13_april_2020.pdf
[2]Xiong TY, Redwood S, Prendergast B, Chen M. Coronaviruses and the cardiovascular system: acute and long-term implications. Eur Heart J. 2020; 41(19):1798–1800.Article Pubmed
[3]National Institute for Health and Care Excellence. COVID-19 rapid guideline: acute myocardial injury. NICE, 2020. Accessed from: https://www.nice.org.uk/guidance/ng171
[4]European Society of Cardiology. ESC guidance for the diagnosis and management of CV disease during the COVID-19 pandemic. ESC, 2020. Accessed from: Website
[5]Mahmud E, Dauerman HL, Welt FG, Messenger JC, Rao SV, et al. Management of acute myocardial infarction during the COVID-19 pandemic: A Position Statement From the Society for Cardiovascular Angiography and Interventions (SCAI), the American College of Cardiology (ACC), and the American College of Emergency Physicians (ACEP). J Am Coll Cardiol. 2020; 76(11):1375–1384.Article Pubmed
[6]Welt FG, Shah PB, Aronow HD, Bortnick AE, Henry TD, et al. Catheterization laboratory considerations during the coronavirus (COVID-19) pandemic. J Am Coll Cardiol. 2020; 75(18): 2372–2375.Article Pubmed
[7]Public Health England. Guidance on social distancing for everyone in the UK. PHE, 2020. Accessed from: https://www.gov.uk/government/publications/covid-19-guidance-on-social-distancing-and-for-vulnerable-people
 Copyright
© 2012-2019 NobleResearch Group. All Rights Reserved
Copyright
© 2012-2019 NobleResearch Group. All Rights Reserved